

Follow-up of drug-coated balloon angioplasty in femoropopliteal disease in a real-world population.
Using drug-releasing devices has decreased the rate of restenosis in obstructive femoropopliteal lesions compared with conventional balloons or conventional stents (bare-nitinol stent, BNS). Both in the placement of BNS and of drug-eluting stents (DES) there is a mechanical risk of stent fracture or aneurysmal degeneration of the treated segment (as reported in some series), so using drug-coated balloons (DCB) could be an alternative to avoid these adverse effects.

The aim of this study was to find out the freedom from restenosis at 1 year after endovascular treatment with DCB for symptomatic femoropopliteal disease.
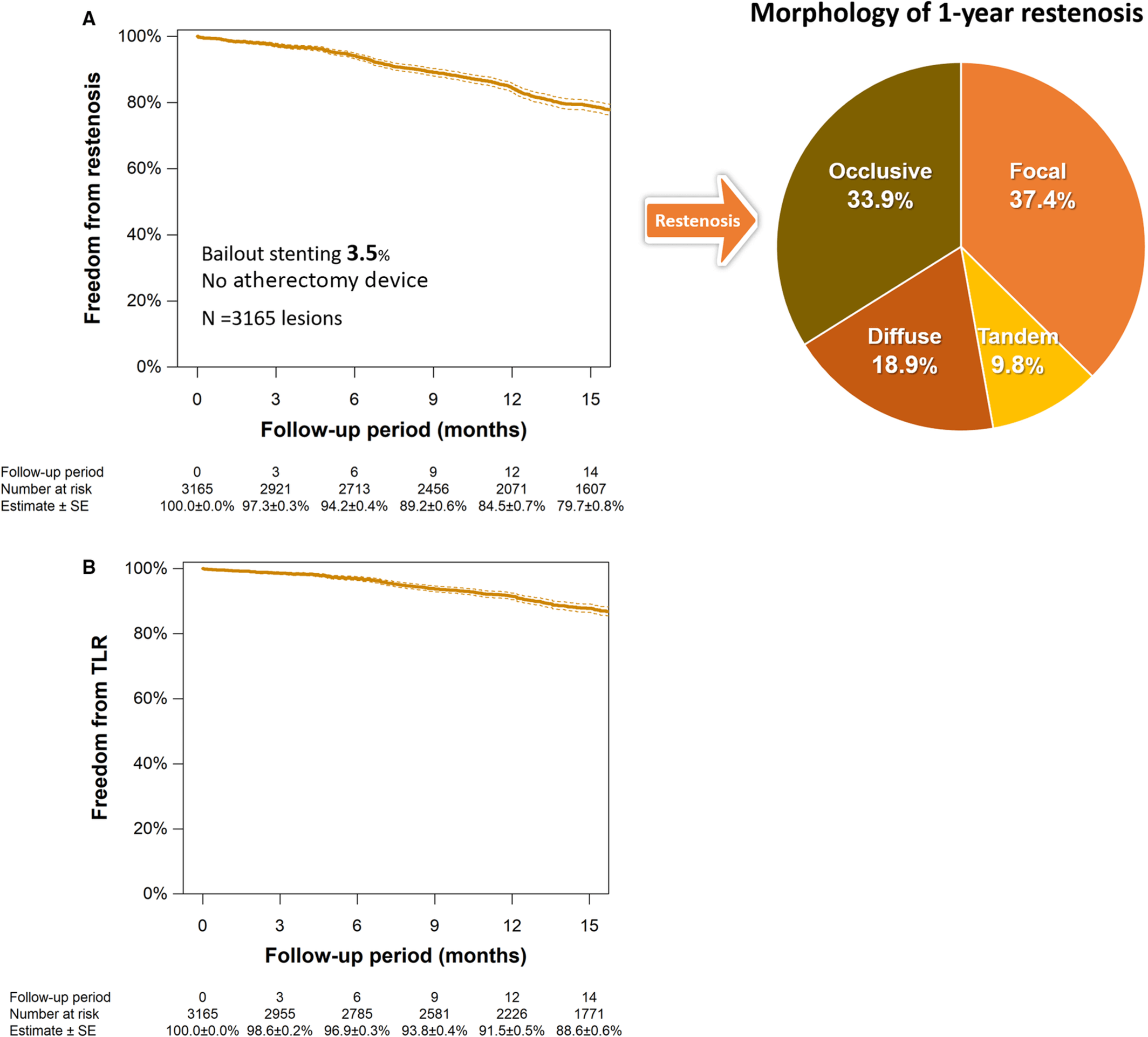
Data for the study was taken from the POPCORN (Prospective Multicenter Registry of Drug-coated balloon for femoropopliteal disease) database from Japan. This country has the particularity of not having authorized the use of atherectomy devices in peripheral disease and the stent bailout strategy is infrequent due to reimbursement policies (only 3.5% of cases).
Predilation was performed 1:1 or 1 mm less, and two types of DCB were used according to operator choice: Lutonix and IN.PACT Admiral.
The primary endpoint was freedom from restenosis at follow-up. The secondary endpoints were freedom from vessel revascularization, limb salvage, freedom from any reintervention, major limb-related adverse effects, and all-cause mortality.
Researchers analyzed 2507 patients with 3165 lesions; mean age was 75±9 years, 64.9% of patients were male, 65.4% had diabetes, and 29% had chronic kidney disease. Clinically, 31.2% of patients presented critical ischemia. Angiographically, the average lesion length was 13.5±9.3 mm, with an average diameter of 4.8±0.9 mm, and 25.9% were chronic total occlusions (CTO). After balloon dilation, 4.6% of patients presented some type of severe dissection, with bailout stenting in 3.5%.
Read also: Should We Use Drug Coated Balloons in Patients with Multivessel Disease?
Follow-up at 14 months was possible for 84.9% of patients (loss to follow-up: 15.1%). Freedom from restenosis was observed in 84.5% of patients (95% confidence interval [CI]: 83.1-85.8%) and in 79.7% of subjects at 14 months (95% CI: 78.1-81.2%), the majority being focal restenosis (37.4%). Freedom from revascularization at 12 months was 91.5% (95% CI: 90.5%-92.5%).
Characteristics independently associated with restenosis at 1 year were history of revascularization (hazard ratio [HR]: 1.32; 95% CI: 1.01-1.73; p = 0.044), severe calcification (HR: 1. 29; 95% CI: 1.03-1.63; p = 0.027), CTO (HR: 1.28; 95% CI: 1.04-1.58; p = 0.021), use of Lutonix (1.97; 95% CI: 1.61-2.41; p ≤ 0.001), and the presence of residual stenosis (HR: 1.51; 95% CI: 1.24-1.83; p ≤ 0.001).
Conclusions
This observational study showed data from a real population treated almost exclusively with DCB (without the use of atherectomy and with a low rate of bailout stenting) that had acceptable restenosis and vessel revascularization rates. Additionally, over two thirds of cases were nonocclusive restenosis. The presence of calcified lesions and of residual lesion were both predictors of restenosis, which should be assessed when choosing DCB in these scenarios.

Dr. Omar Tupayachi.
Member of the editorial board of SOLACI.org.
Original Title: Vessel Patency and Associated Factors of Drug‐Coated Balloon for Femoropopliteal Lesion.
Reference: Soga Y, Takahara M, Iida O, et al. Vessel Patency and Associated Factors of Drug-Coated Balloon for Femoropopliteal Lesion. J Am Heart Assoc. 2023;12(1):e025677. doi:10.1161/JAHA.122.025677.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



{kind=link}