

Original Title: 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease. Reference: Levine GN et al. Circulation. 2016 Mar 29. [Epub ahead of print].
Courtesy of Dr. Alejandro Lakowsky.
The new ACC-AHAGuidelines on the optimal duration of dual antiplatelet therapy(DAPT) in patients with coronary artery disease have just been published in Circulation online.
The document updating 6 previous guidelines on this matter wasreleased along with a thorough analysis ofthe informationavailable. A systematic review on the existing evidence conducted by the same team of physicians was published together with the new recommendations.
Right about now, JAMA online has released the DAPT score, one that helps identify the patients that will benefit from a more prolonged DAPT, which had been anticipated as an abstract at the AHA Meeting in November 2015.
What is new about the ACC-AHA guidelines:
- The guidelines style has been updated to make it easier to read; it has shorter explanations of the reasons behind these recommendations, which use to be extensive in prior guidelines. It has incorporated the new Class of Recommendation (CoR) and Level of Evidenced (LoE) classifications, that started 3 years ago with Class III, divided in two subclasses (“no benefit” and “harm”), and continued in 2015, when LoE B was subdivided in two (evidence of randomized or non-randomized studies) and LoE C (evidence based on limited data or on experts’ opinions).
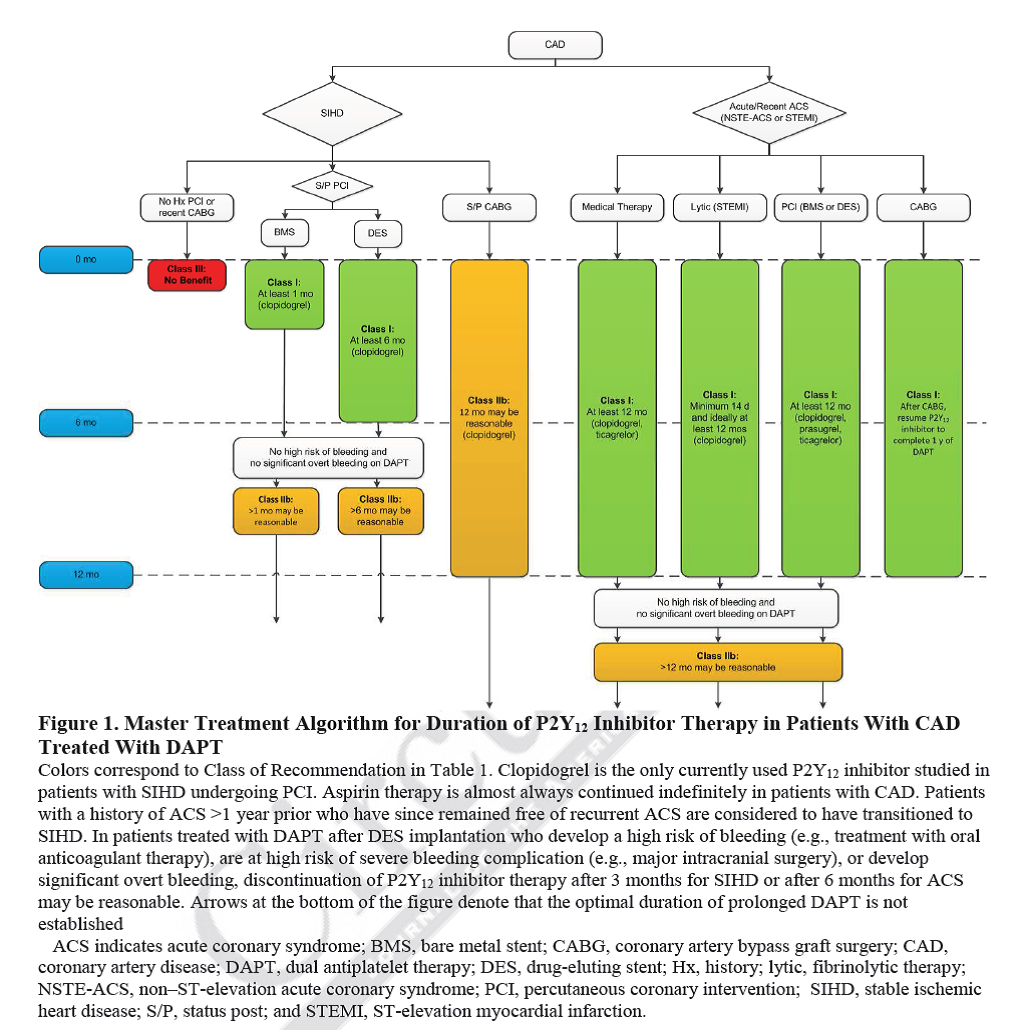
- Recommendations on the post PCI use of DAPT in these guidelines are based on the new drug eluting stents (DES), not on first generation stents. Generally speaking, these recommendations do not include patients requiring chronic oral anticoagulation. More modern stents are known to have better results than bare metal stents (BMS) in nearly all clinical situations and with lower rates of stent thrombosis risk.
- In general, a CoR I is given for the mandatory period of 6 to 12 months of DAPT post PCI (12 months in case of acute coronary syndrome) and aCoR IIb for prolonged DAPT after this period.
- The recommended DAPT period of 12 months is reduced to 6 in PCI with elective DES (programed PCI) (CoR I), with the option to use more or less than 6 months (CoR IIb) for patients with low or high bleeding risk, respectively. Many experts believed the previous recommendation of 12 months was unfounded and that there was no solid evidence to support it; 6 months appeared more reasonable (and this period could be even shorter with certain kind of stents under certain clinical situations, such as high bleeding risk patients). It is worth clarifying this does not apply to acute coronary syndromes (SCA), or to patients with first generation stents.
- Always use low doses of aspirin. The recommended dose is 81 mg/day (range: 75-100 mg/day).
- The recommendations are unified for all ACS, with no distinction between STEMI and NSTEMI ACS,given that both syndromes belong to the same clinical spectrum.
- The preference of ticagrelor or prasugrel over clopidogrel in ACS receives aIIarecommendation.
- With candidates for prolonged DAPT (> 6-12 months), the optimal duration is still unknown.
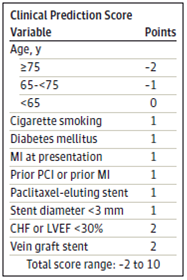
- The guidelines mention certain criteria included in theDAPT scoreto help identify good candidates for prolonged DAPT: subjects with ACS, diabetic, smokers, a history of infarction or PCI, cardiac failure or severe systolic dysfunction, PCI to a venous graft and stents of small diameter (< 3 mm). It is worth noting that regarding the prolonged use of dual antiaggregation in the DAPT score, age has an inverse correlation with benefit (patients younger than 65 see more benefits).
- Emphasis is placed on the fact that this guidelines provide general recommendations only and that physiciansshould carefully assess each particular case when deciding on the most adequate strategy. In many cases, optimal DAPT duration is unknown.
- This is the general algorithm (there are several tables with particular algorithms, including recommendations for post CABG patients):
News on the JAMA issue on DAPT score:
- In contrast to the presentation at AHA 2015, where the score was criticized over the fact that it had no external validation, this issueincorporates a validation cohort with more than 8,000 patients from the PROTECT trial.
- The authors chose to make one single score contemplating variables that predict ischemic and bleeding risk, over two different score systems for each event.
- The score ranges from -2 to 10. A score equal or higher than 2 identifies patients with high ischemic risk and not such a high risk of bleeding that would benefit from prolonged DAPT.
- The score has poor discrimination power (statistic C of 0.70 and 0.68 to predict bleeding or ischemic events, respectively; in the PROJECT validation cohort, these values were even lower, 0.64 in both cases). Although this tool seems potentially useful, it needs to be perfected and confirmed by other studies.
Courtesy of Dr. Alejandro Lakowsky.
MTSAC.



{kind=link}