

Courtesy of Dr. Agustín Vecchia.
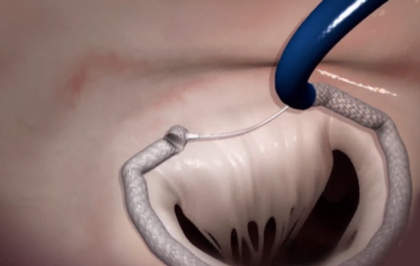 In the last few years, new percutaneous treatment options for mitral regurgitation have emerged. Transcatheter mitral annuloplasty with various devices is a relatively simple procedure that could compress the origin of circumflex artery branches due to the different orientation of mitral corners and the coronary sinus.
In the last few years, new percutaneous treatment options for mitral regurgitation have emerged. Transcatheter mitral annuloplasty with various devices is a relatively simple procedure that could compress the origin of circumflex artery branches due to the different orientation of mitral corners and the coronary sinus.
The following work by Park et al. presents the first human test for a “percutaneous mitral cerclage” device that would offer the advantage of tensing the annulus, protecting entrapped coronary arteries from compression.
The study enrolled 5 patients with functional class III/IV mitral regurgitation receiving complete medical treatment as per guideline recommendation, who presented one of the following echocadiographic parameters:
- Effective regurgitant orifice area (EROA) >0.20 cm2
- Regurgitant volume >30 mL
- Regurgitant fraction = 50%
- During the procedure, the left subclavian veins and some of the femoral veins are first cannulated. By means of subclavian access, the coronary sinus and the great cardiac vein are identified through a venography.
- Then, a 0.014” wire (Whisper, Abbott, Chicago, Illinois) is used to place a microcatheter (Crusade, Kaneka Medix, Osaka, Japan) in the basal septal perforator vein, through which the interventricular septum is crossed with a hard-tip wire in order to reach the right ventricular outflow tract.
- Through a specific device, the wire is captured in the right ventricular outflow tract and externalized through femoral access; then it is recaptured and externalized towards the subclavian vessel by means of a loop.
- The cerclage system is lowered and a coronary protection system is put in place with extreme precision through coronarography.
- Finally, the cerclage system is tensed and the mitral annular diameter is consequently reduced. This step is monitored through transesophageal echocardiography to obtain the optimal closure degree. The tensing device is fixed subcutaneously in a pocket similar to that for a pacemaker.
The primary outcome of this work was mitral regurgitation severity after one month. The safety outcome was a lack of major adverse cardiovascular events (MACE: death, acute myocardial infarction, cardiac tamponade, device-related surgery, stroke, or electrocardiogram [ECG] conduction disorders) after one month. The procedure was successful in 4 out of 5 subjects and not performed in 1 of them due to atypical vein anatomy. Patients received dual antiplatelet therapy (DAPT) with aspirin and clopidogrel for at least 3 months.
- Cerclage impact on cardiac chambers and mitral regurgitation: The procedure reduced the mitral annular diameter by 14% as determined through echocardiography. Both regurgitant volume and EROA decreased at the time of the procedure, and kept decreasing at 6 months of follow-up (with reductions of 66% and 76% at 6 months, respectively). Cardiac chamber dimensions also decreased at 6 months: 34% for the left atrium, 31% for the left ventricular end-diastolic volume index, and 31% for the left-ventricular end-systolic volume index. There was also a persisting significant reduction in tricuspid regurgitation.
- Atrial fibrillation: Two patients, one with persistent atrial fibrillation and one with permanent atrial fibrillation reverted to sinus rhythm after the procedure. This happened during the procedure in one patient, and at 3 months in the other. One patient with paroxysmal atrial fibrillation before the procedure did not present episodes during 6 months of follow-up.
- Safety outcome: One of the four patients experienced a small myocardial infarction due to small obtuse marginal branch coronary occlusion. One subject experienced right bundle branch block considered as secondary to interventricular septum traction from the device. There were no instances of atrioventricular block.
The authors conclude that this feasibility study is positive, and they highlight the importance of further research on this technique.
Editorial
This study features a very limited number of patients, but it still achieves its purpose of showing the feasibility of this new device for the treatment of functional mitral regurgitation. The results for this procedure are promising and its safety parameters are acceptable. Whether any of these treatments is better than the current standard of care (optimal medical treatment, coronary revascularization, and cardiac resynchronization therapy [CRT]), in this heterogeneous patient group, remains to be seen. The COAPT study (ongoing), comparing Mitraclip vs. standard of care, may provide the answer and kickstart future randomized studies with this and other innovative devices.
Courtesy of Dr. Agustín Vecchia. Buenos Aires German Hospital, Argentina.
Original title: Mitral Loop Cerclage Annuloplasty for Secondary Mitral Regurgitation First Human Results.
Reference: 10.1016/j.jcin.2016.12.282 JACC Cardiovascular Interventions.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}