

Coronary bifurcation angioplasty remains one of the most frequent and technically challenging scenarios in interventional cardiology. Between 15% and 20% of coronary procedures involve bifurcation lesions, whose treatment carries risks including stent malapposition, carina shift, dissection, or occlusion of the side branch (SB). In this setting, the provisional single-stent strategy has become the preferred approach for most lesions. Contemporary technique includes stent sizing according to the distal main vessel diameter and systematic proximal optimization technique (POT).
However, once the stent has been implanted in the main vessel and POT has been performed, debate persists regarding whether the SB should be systematically treated. The aim of the KISS study was to evaluate whether a conservative strategy (without SB intervention) could be non-inferior to a strategy involving systematic SB intervention.
A randomized, prospective, open-label, multicenter international study (conducted in European centers) enrolled 616 patients with non-left main coronary bifurcation lesions. Patients were treated with Resolute Onyx stents in the main vessel. Following POT, and after confirming the absence of SB occlusion or flow deterioration, patients were randomized 1:1 to either no SB intervention or systematic SB intervention. Left main lesions, planned two-stent strategies, STEMI, cardiogenic shock, TIMI flow < III in the SB, and left ventricular ejection fraction <20% were excluded.
The primary endpoint was the occurrence of periprocedural myocardial infarction or significant myocardial injury according to ARC-2 criteria.
Read also: Complex radial access: a four-step protocol to overcome loops and tortuosity.
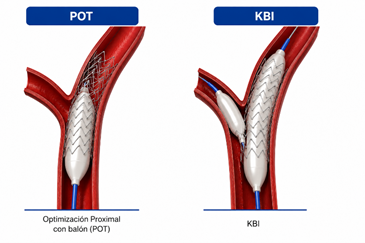
The mean age was 67.7 years, and 81% of patients were treated for chronic coronary syndrome. The most frequent bifurcation site was the left anterior descending artery–diagonal branch. In the conservative group, only 2% required bailout SB intervention. In the systematic intervention group, 57% underwent isolated SB balloon dilation (typically POT-Side-POT) and 43% underwent kissing balloon inflation (KBI). SB stenting was required in 5.8% of systematically treated patients.
The primary endpoint occurred in 4.1% of patients without SB intervention versus 5.7% of those undergoing systematic SB intervention, meeting the criterion for non-inferiority (p<0.001), although superiority was not demonstrated (p=0.38). No significant interactions were observed according to age, sex, Medina classification, or degree of residual SB stenosis.
The conservative strategy was associated with simpler procedures, shorter procedural time (34 vs 45 minutes; p<0.001), reduced fluoroscopy time (10 vs 13.2 minutes; p<0.001), and lower radiation exposure. Complications were infrequent; however, SB dissection was significantly more common in the systematic intervention group (2.9% vs 0%; p=0.004).
At 12 months, no differences were observed in clinical outcomes such as target lesion failure (4.9% vs 6.4%; p=0.442) or definite/probable stent thrombosis (0.7% vs 0.6%; p=0.971). Improvement in angina symptoms was greater in the group without systematic SB intervention (99.0% vs 93.7%; p=0.040).
In selected patients with non-left main coronary bifurcation lesions, the contemporary provisional stenting strategy with systematic POT and no routine SB intervention proved non-inferior to systematic SB intervention regarding periprocedural myocardial infarction or significant myocardial injury. These findings support a simplified strategy, avoiding additional SB interventions when no significant angiographic compromise is present.
Original Title: Side Branch Additional Treatment for Coronary Bifurcation Lesion Revascularization: Insights From the KISS Randomized Trial.
Reference: Chevalier, B, Cornillet, L, Bouisset, F. et al. Side Branch Additional Treatment for Coronary Bifurcation Lesion Revascularization: Insights From the KISS Randomized Trial. J Am Coll Cardiol Intv. 2026 Apr, 19 (8) 961–972. https://doi.org/10.1016/j.jcin.2026.02.012.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



{kind=link}