


In keeping with its Clinical Case Discussion Program, SOLACI’s peripheral interventions department, SOLACI Peripheral, presents the third clinical case, to promote knowledge exchange across the entire Latin American hemodynamics community.
Share your thoughts on case and resolution in the comments and answer the questions at the end of the article.
Femoral PCI
Authors: MD Mauricio Cavalieri Machado / MD Caiser T. S. Junior / MD Thiago José de Assis
Contact: mcavmachado@gmail.com
Healthcare center: Luxemburgo Hospital, Belo Horizonte/ MG. Brazil.
– Patient: 75-year-old woman. Stenting of right and left femoral arteries in 2018.
– Patient informs intermittent claudication after 100 m walk is back, with pain in lower right and left limbs (Fontaine IIB, Rutherford 4).
– History of hypertension, hypothyroidism, dyslipidemia, and atrial fibrillation. Use of losartan 50 mg BID, amlodipine 10 mg MID, simvastatin 40 mg MID, Hidantal, rivaroxaban 20 mg MID, amiodarone, Puran t4 75 mcg/day, fluoxetine 20 mg/day.
– Lower limb echo-doppler shows new occlusions in both femoral arteries. Distal bed is good.
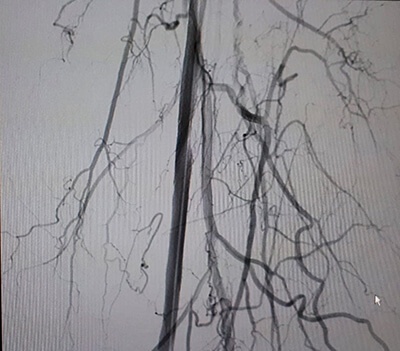
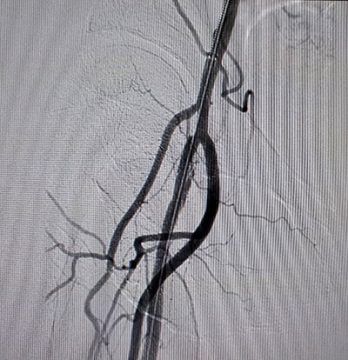
These are the angiography images. TASC D occlusions.
Left lower limb
-

1- Left SFA occlusion proximal to stents. -
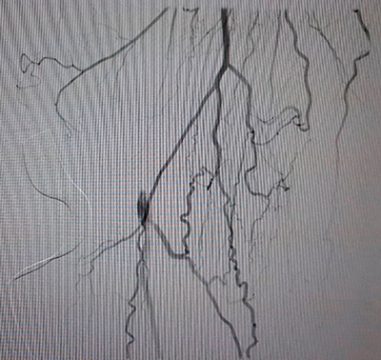
2- Collateral of popliteal -
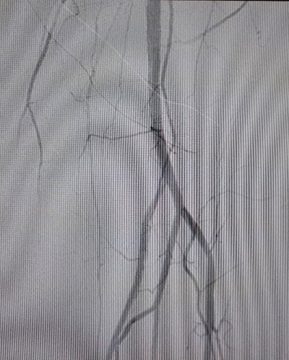
3- Good distal bed
Right lower limb
-
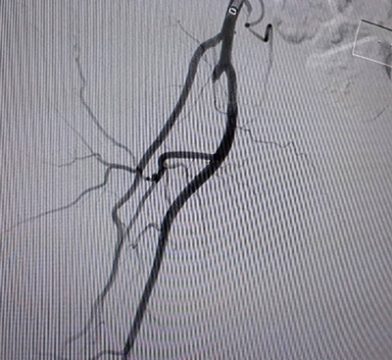
4- Occlusion proximal to stents -

5- Collateral of popliteal -
6- Good distal bed
Question… What course of action should we recommend?
Case Solution
– We treated both lower limbs percutaneously. We stopped using rivaroxaban and started ASA and clopidogrel 48hrs before procedure.
– To treat the left SFA, we performed a contralateral retrograde right CFA puncture and placed a 6F sheath, 45 cm long. We attempted crossing proximal occlusion into stent lumen, but the guidewire would go to false lumen.
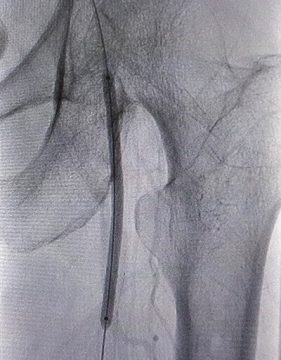
– We then opted for distal SFA approach, with a 4F inductor and retrograde puncture through the thigh.
-

7- Fluoroscopy guided needle placement -

8- Retrograde distal left SFA access with 4F sheath. -

9- Retrograde distal left SFA access with 4F sheath.
– We crossed the occlusion and exteriorized the guidewire
– We performed balloon dilation and successfully completed with drug coated balloon.
-
10- Balloon -
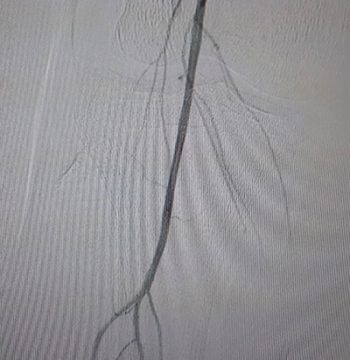
11- Restored flow
– One month after first intervention, we treated the right SFA.
– We now puncture the left CFA using contralateral femoral sheath placement. We successfully penetrated proximal stent occlusion but when exiting, there was vessel dissection and the guidewire stayed in false lumen, which prevented advancing along the popliteal.

– Once more we opted for the retrograde approach in leg. This time punctured the anterior tibial artery (images 13, 14), advanced the 0,014 guidewire in a retrograde fashion, and exteriorized it (video 2).
-
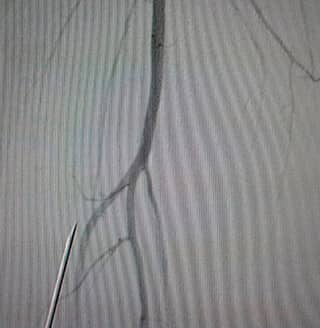
13- Fluoroscopy guided needle positioning -

14- 0,014 guidewire with OTW balloon through proximal access of the anterior tibial artery
– Guidewire snaring.
– Balloon dilation successfully completed with drug coated balloon (images 15,16).
-
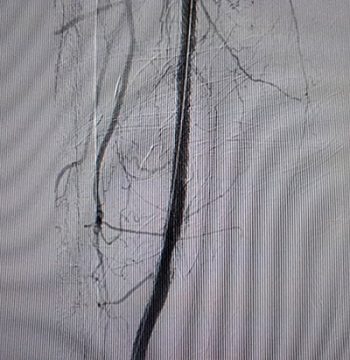
15- Right SFA flow restored. -
16- Proximal right SFA segment (final outcome)
Devices used:
- 6F Sheath
- 4F Sheath
- 0,035 260 cm stiff hydrophilic guidewires
- IM catheter
- Long sheath 50 cm Destination
- Oceanus 35 4 X 80 and 5 X 150 balloon
- 3,5 X 60 OTW balloon
- Admiral 6 X 150 cm paclitaxel coated balloon
- 0,014 PT2 300 cm guidewire
- 5F Glidecath catheter
Question: what measurements would you use to prevent repeat stent thrombosis?
Conclusions
- Endovascular treatment can be used in TASC A to D lesions
- The most popular bailout technique for challenging rechannelization is the retrograde approach which, in addition to good outcomes, has excellent cost-benefit ratio.
- Drug coated balloons can be used for stent restenosis.
Discover other SOLACI Peripheral clinical cases
Get the latest scientific articles on interventional cardiologySubscribe to our weekly newsletter
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}