


SOLACI’s Department of Peripheral Endovascular Interventions brings a new challenging clinical case for the whole Latin American medical community so as to continue fostering and sharing scientific knowledge and experience among peers.
Tell us what you think about this case and its resolution using the comments section in this post, and answer the questions featured in the last part of this article.
Juxtarenal Abdominal Aortic Aneurysm
Authors: Dr. Luis R. Virgen Carrillo, MD, PhD / Dr. Carlos Salazar, MD / Dr. Rodolfo Siordia Zamorano, MD.
E-mail: drvirgen@cardiovascular.mx; Twitter: @drluisvirgen
Institution: Virgen Cardiovascular Research, Guadalajara, Mexico, & Cirujanos Cardiovasculares del Noroeste.
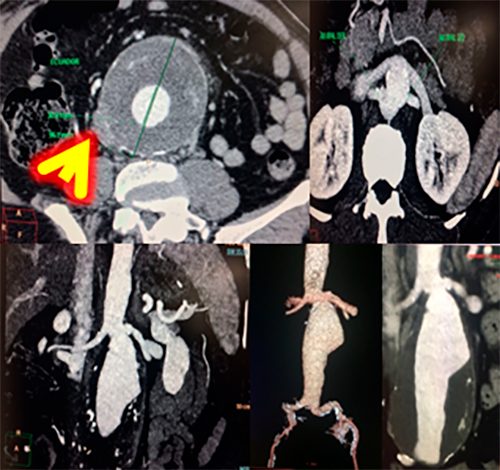
– Male patient, 61 years old, anesthesiologist, cigarette smoker, hypertensive. He begins experiencing intense abdominal pain. Hb reduction, 14-11 g/dL. He is hemodynamically stable; blood pressure 110/60 mmHg, heart rate 68 bpm. An abdominal computed tomography angiography shows the contained rupture of an abdominal aneurysm. Anatomy: juxtarenal aneurysm without neck, with small, tortuous iliac arteries.
Case Resolution
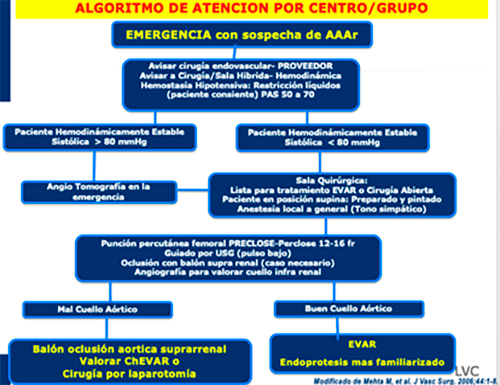
– The algorithm for the attention of patients with suspected abdominal aneurysm rupture is activated. Physicians choose a percutaneous endovascular treatment (the chimney technique [chEVAR]).
– The procedure is conducted in a hybrid cath lab; bilateral femoral artery puncture, guided by ultrasound and image fusion. Two Perclose devices are used in each femoral artery. Both brachial arteries are dissected; an 8-Fr flexor introducer sheath is placed inside each renal artery. Selective renal artery catheterization and stenting using an 8×39 film-coated BeGraft (Bentley Innomed GmbH, Hechingen, Germany). A parallel 0.035” Magic Torque guidewire ×260 cm is used. Then, an Ovation 26 Abdominal Stent Graft System (Endologix, California, USA), 14-15 Fr OD, is used. The device is placed using image fusion, the fill polymer is delivered, and both BeGraft stents are implanted. After the procedure, there is a type Ia endoleak in peri-chimney spaces (“gutters”). New dilation conducted with partial improvement. A decision is made to conduct an embolization with an Onix device at a second instance.
– The patient is stable and does not experience pain. An ultrasound is conducted within 24 hours: no flow in the aneurysm sac.
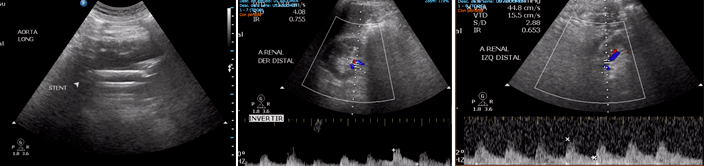
– A computed tomography angiography is conducted at 72 hours, 1, 6, and 12 months; no endoleaks. (VIDEO #2)
Questions
- Is there an algorithm for the attention of patients with suspected abdominal aneurysm rupture at your site?
- In your opinion, what is the best option for a patient with aneurysm rupture: surgical treatment or endovascular treatment?
- What is your treatment of choice for para/juxtarenal aneurysms?
- Should type I endoleaks be treated in the cath lab?
Join the conversation through the comments in this post!
Get the latest scientific articles on interventional cardiologySubscribe to our weekly newsletter
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}