


A new clinical case to keep learning with colleagues!
Today, we present a Thoracic Aortic Dissection in Patient with Complex Arch. This is the 4th case for SOLACI Peripheral, which continues its mission: to deepen knowledge exchange among Latin American interventional cardiologists.
Tell us what you think about this case using the comments section in this post, and answer the questions featured in the last part of this article.
Thoracic Aortic Dissection in Patient with Complex Arch
Authors: Felix Damas de los Santos, MD. Eduardo A. Arias Sánchez, MD. Mauricio Soule Egea, MD
E-mail: damasdelossantos@yahoo.com.mx, Twitter: @felixdamasds
Site: Angeles Acoxpa Hospital, Mexico City, Mexico. Ignacio Chávez National Cardiology Institute, Mexico City, Mexico.
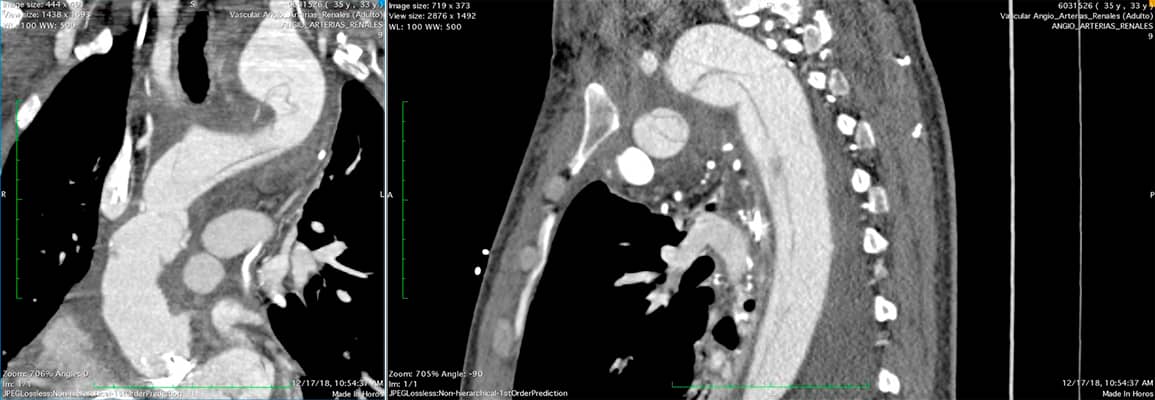
33-year-old male patient with Ehlers-Danlos syndrome, prior hemorrhagic stroke in 2008 (which required an embolization), and multiple atlas and lumbar fractures.
Patient experiences chest pain and dyspnea. A Stanford type A and DeBakey type I thoracic aortic dissection is documented, with severe aortic and mitral regurgitation. His CT imaging is as follows:

Given the context, what would you choose?
- Surgical intervention.
- Endovascular treatment.
- Another option.
If you were to conduct a surgical intervention, which surgical path would you take?
- Aortic valve replacement + mitral valve replacement + Complete repair of ascending aorta and arch with reimplantation of supra-aortic vessels.
- Mitral valve replacement + Bentall-De Bono procedure.
- Another option.
The patient undergoes a successful mitral valve replacement and Bentall-De Bono procedure (ascending aorta repair with aortic valve replacement).
After removing the mechanical ventilation support 24 hours after the procedure, the patient experiences an 8-9/10 persistent chest pain. CT imaging shows dissection expansion.
At this point, it is decided to…
- Conduct a complete endovascular treatment.
- Perform a revascularization of supra-aortic vessels + endovascular treatment at a second instance.
A decision is made to revascularize supra-aortic vessels to prepare for an endovascular repair. Post-revascularization control imaging showed the following findings.
On and off chest pain continues.
Endovascular procedure: Right femoral surgical approach and right radial percutaneous approach with 7-6 Fr Slender.
Multipurpose catheter with a 300-cm hydrophilic guidewire, then exchanged for a pigtail catheter. An angiography is conducted.
The device is later exchanged for a Lunderquist guidewire. The aortic graft and supra-aortic vessels are reached through transradial access to mark the landing zone.
Initially, a Relay prosthesis (34-162 mm) is inserted. During insertion, resistance is felt.
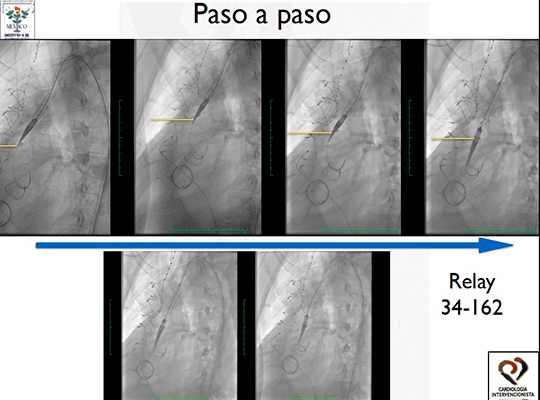
Given the resistance:
- You change it for another prosthesis adapted to planned measures, or
- You stick to the same model.
Physicians decide to insert a Valiant 32-204 prosthesis.
At first, the prosthesis cannot be inserted, so a Relay 32-114 is used and positioned.
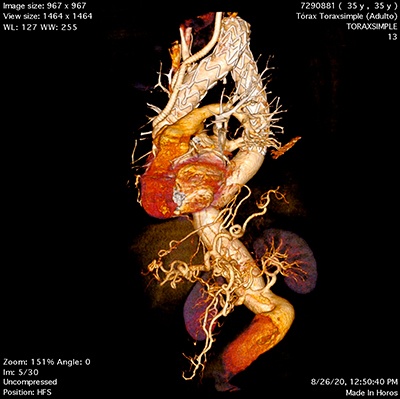
Ultimately, the Valiant prosthesis is positioned within the descending aortic artery. The final result is shown.
The final video shows the follow-up image 1 year after the procedure. FIGURE 3.
Taking into account the diagnostic TC imaging and considering the patient’s anatomical characteristics:
Which treatment possibilities would you have considered?
- Complete surgical approach: aortic mitral valve replacement and complete surgical aortic arch repair.
- Mitral valve replacement and Bentall-De Bono procedure, outcome assessment and complete arch endovascular treatment.
- Mitral valve replacement and Bentall-De Bono procedure, and simultaneous supra-aortic vessel revascularization.
- Mitral valve replacement, Bentall-De Bono procedure, revascularization at a second instance, and endovascular treatment as a third instance.
Elaborate on your choice in the comments section of this article.
Discover other SOLACI Peripheral clinical cases
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}