


SOLACI’s Department of Peripheral Endovascular Interventions is promoting the analysis of challenging clinical cases on peripheral interventions so as to foster the participation and engagement of all SOLACI members.
In this first issue, we present a clinical case around carotid artery stenting.
Read thoroughly the case below and take part in an unrestricted discussion through the comments below this post.
A case of carotid artery stenting Carotídea
– 74-year-old male patient.
– Reports of intense vertigo requiring rest, unrelated to exertion.
– History of high blood pressure.
– Left carotid bruit found during physical examination.
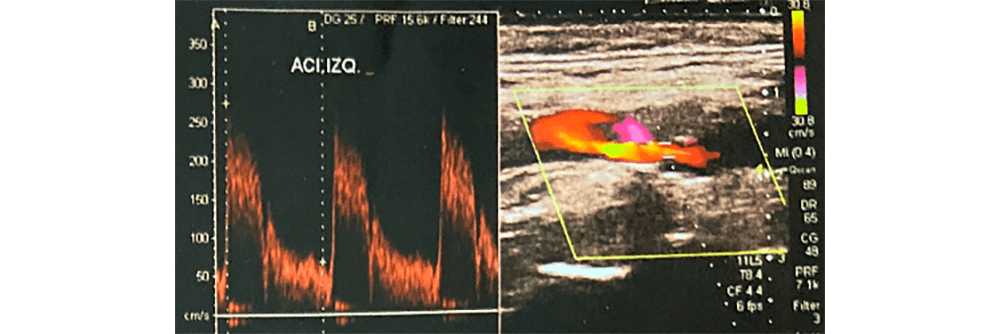
– Carotid artery Doppler echocardiography (figure 1), left internal carotid artery, fibrocalcific plaque, 70% stenosis.
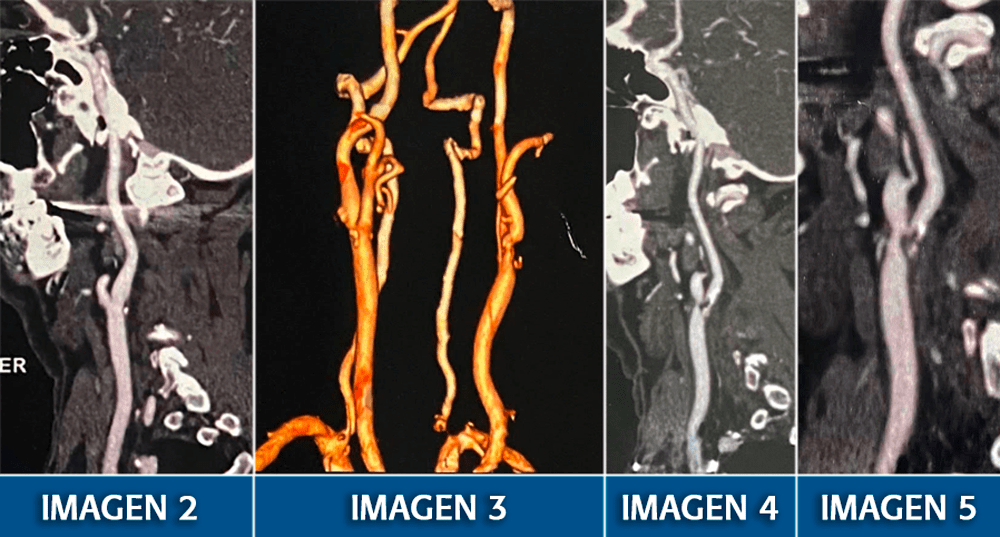
– Carotid artery computerized tomography (CT) angiography: right external and common carotid arteries without lesions; internal carotid artery with small calcified plaque and mild stenosis in the carotid sinus area. (Figure 2. Figure 3 in 3D).
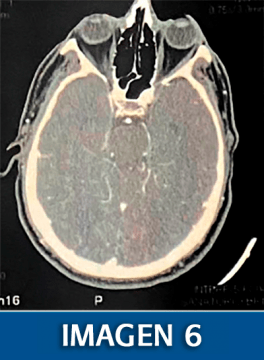
– Brain CT: no significant lesions (figure 6).
– Aortic arch aortography: no stenosis, type 1 arch.
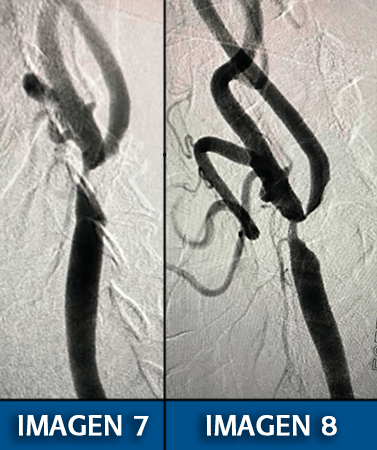
– Carotid artery arteriography: the right common carotid artery correlates with the description derived from the CT angiography. Left common carotid artery distal third, 80%, and left internal carotid artery, sub-total (figures 7-8 and video 1).
Questions
- Do you expect the patient to be symptomatic?
- Would you indicate revascularization? Would you perform an endarterectomy or a percutaneous intervention?
- Should you choose a percutaneous procedure, which catheterization system would you choose? Which filter? Which stent?
Join the conversation through the comments in this post!
Left internal carotid artery angioplasty:
– Selective left common carotid artery cannulation with 8-Fr JR 3.5 guidewire over 0.035 hydrophilic sheath.
– Handling of 0.014 guidewire through left internal carotid artery lesion and distal positioning. Crossing and opening of 5.5 Spider filter. (Figure 9).

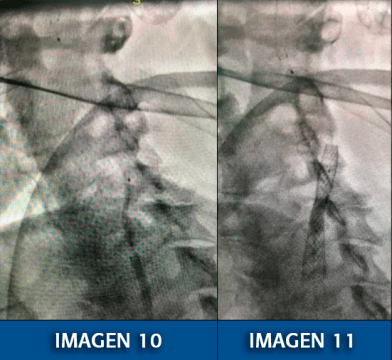
– Balloon predilation 3.0 × 20 mm, at 8 atmospheres. (Figure 10).
– Placement and release of self-expanding stent Carotid Wallstent 9.0 × 30 mm.
– Balloon post-dilation 6.0 × 20 mm at 8 atmospheres (figure 11).
– Filter retrieval 7:10 minutes after its opening.
– Final result (figure 12 and video 2), 20% residual lesion, no complications.

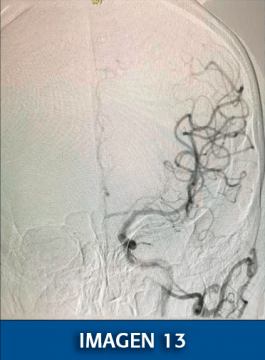
– Preserved intracerebral angiographic control (figure 13).
Courtesy of Dr. Daniel Aníbal Zanuttini.
Discover other SOLACI Peripheral clinical cases
Get the latest scientific articles on interventional cardiologySubscribe to our weekly newsletter
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}