


Here is a new SOLACI PERIPHERAL Case!
In this opportunity, Dr. Ana Paula Mollón (Arg.) presents “Common, Superficial and Deep Femoral Artery Recanalization”. This is the 6th clinical case presented by SOLACI Peripheral. The purpose of this space is to encourage and further the exchange of experiences and opinions, to keep advancing our knowledge in interventional cardiology.
Take part in the discussions and leave your comments!
Common, Superficial and Deep Femoral Artery Recanalization
Authors: Dr. Ana Paula Mollón (ARG)
Contact: anapaulamollon@gmail.com. Twitter: @anamollon.
Institution: Clínica CEMEP.
Discover other SOLACI Peripheral clinical cases
Background
- 72-year-old male
- CRF: former heavy smoker
- Diabetes
- Dyslipidemia
- CABG in 2016.
Background to the current disease: bilateral claudication with good evolution after medical treatment and exercise.
During lockdown, worsening of left leg.
The patient stops walking. Gains 10 kg.
Starts to feel pain at rest.
Physical exam: absence of distal pulse
Lower temperature in left leg
Strategy
- Contralateral retrograde access
- cross-over 6 Fr inductor
- Hydrophilic 0.035” Stiff Glidewire.
- Vertebral Hydrophilic Catheter
- Distal retrograde access for recently
- Guidewire 0,014” 300 cm V14.
- Guidewire 0,018” 300 cm Command 18.
- Balloon diameters 5 x 150 mm 6 x 150 mm NC 7 x 80 mm.
- Supera 5.5 x 200.
- Supera 5.5 x 150.
- Supera 6.5 x 80.
Questions
- What technique would you use to treat the bifurcation?
- Would you have considered recanalization of deep femoral only? Or would you have used the surgical technique?
Technique
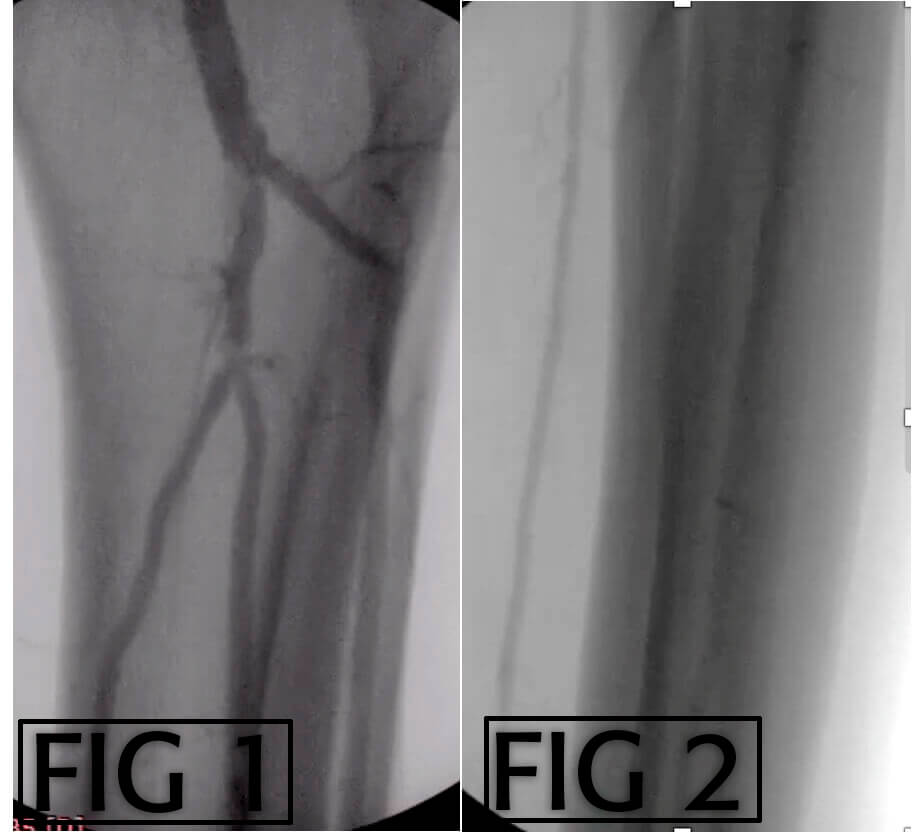
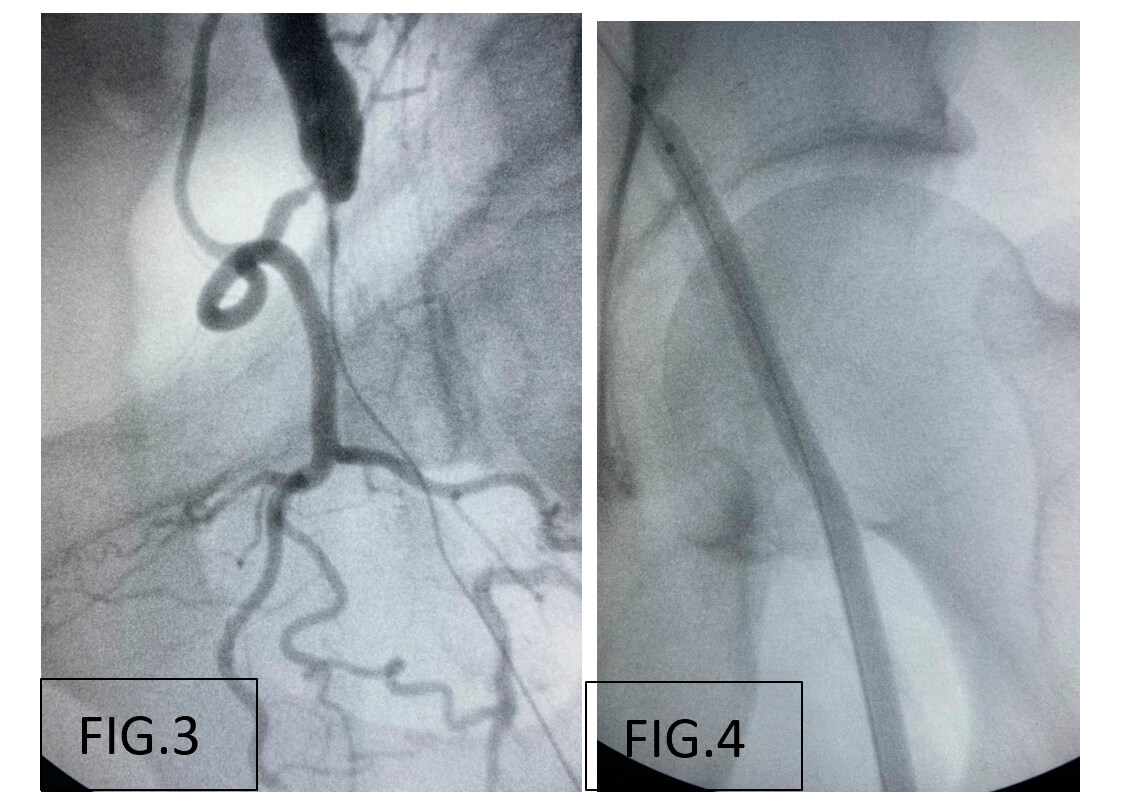
- Common and deep femoral recanalization with anterograde hydrophilic guidewire 0.035”. Progressive balloon angioplasty with 4.0 x 100 mm and 5.0 x 150 mm balloons.
- Recanalization of subintimal proximal superficial femoral and reentry in true lumen.
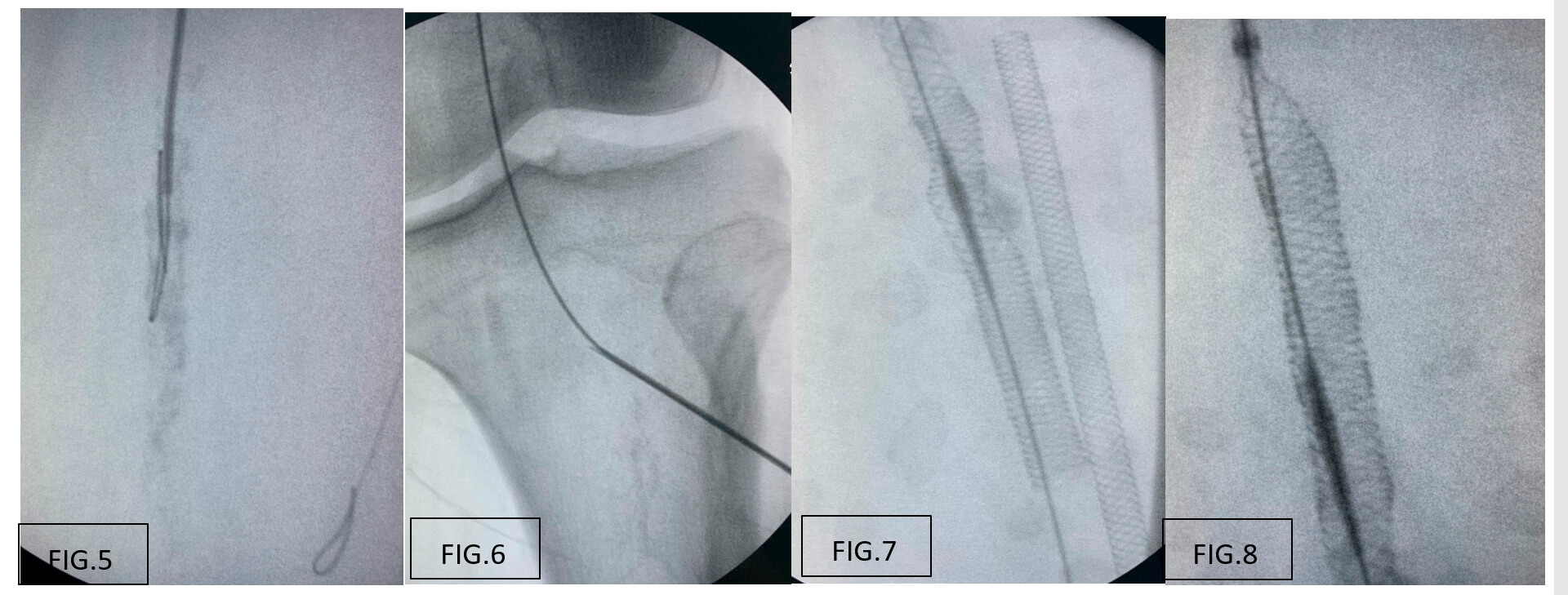
- Anterograde attempt to rechannel more distal occlusion; failure due to severe calcification; distal access through distal popliteal (P3) with 18G puncture needle 0.018” guidewire. Connection of both vessels through vertebral catheter 5F. progressive balloon angioplasty with 4.0 x 100 mm and 5.0 x 150 mm, and 6.0 x 150 balloons and 6.0 x 60 non-compliant balloon.
- Endovascular hemostasis with distal access balloon for 7 minutes.
- Mimetic stent implantation.
- Final result.
Images of the Procedure
– Anterograde recanalization of common and deep femoral with hydrophilic guidewire. Progressive balloon angioplasty with 4.0 x 100 mm and 5.0 x 150 mm balloons.
– Proximal superficial femoral recanalization and reentry in true lumen.
– Anterograde recanalization attempt of more distal occlusion; failure due to severe calcification; distal access via distal popliteal (P3) with 18G punction needle and 0.018” guidewire and connection of both vessels through catheter.
– Vessel prep with balloons of escalating diameter up to 6.0 and 7 in common femoral with supera stent implantation 5.5 in SFA and 6.5 in CFA.
Final Result
Discover other SOLACI Peripheral clinical cases
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



{kind=link}