

Share your experience. Learn from experts. Grow as an interventional cardiologist.
A new edition of the Fellow’s Corner is here, an academic exchange space designed for fellows to share real-world clinical cases, discuss therapeutic strategies, and analyze the main challenges of contemporary cardiovascular intervention.
On this occasion, we present a clinical case accompanied by a series of interactive questions that encourage reflection on decision-making in complex scenarios. At the end, we will share the case resolution and the strategy that was ultimately implemented.
In this second edition, we address an uncommon yet highly impactful clinical situation: “Acute Myocardial Infarction Due to Simultaneous Occlusion of Two Coronary Arteries.”
- Case Authors: Dr. Lorena Anahí Barrera Pérez (Mexico), Dr. Oscar Manuel Granados Casas, Dr. Julio César Mayén Casas.
- Institution: Regional Hospital “1° de Octubre” – ISSSTE.
- Department Chief: Dr. González Coronado Vidal José.
Table of Contents
- Case Presentation: Acute Myocardial Infarction Due to Simultaneous Occlusion of Two Coronary Arteries
- Multiple Choice Questions
- Case resolution
Case Presentation: Acute Myocardial Infarction Due to Simultaneous Occlusion of Two Coronary Arteries
Clinical Data and Medical History
- Type 2 diabetes mellitus diagnosed 2 years ago, treated with Metformin 850 mg every 24 hours.
- Systemic arterial hypertension diagnosed 2 years ago, treated with Enalapril 10 mg every 24 hours.
- Substance use: chronic daily alcohol consumption for 49 years, with frequent episodes of intoxication.
- Remaining relevant medical history: denied.
Medical History
- Patient with a history of Class III chronic coronary syndrome.
- Reports an acute myocardial infarction in 2022 without undergoing angioplasty. He was receiving Atorvastatin 20 mg every 24 hours, Clopidogrel 75 mg every 24 hours, and Metoprolol 100 mg every 24 hours, although without subsequent medical follow-up.
Cardiovascular Risk Factors
- Age, male sex, sedentary lifestyle, alcohol abuse, chronic coronary syndrome, type 2 diabetes mellitus, and systemic arterial hypertension.
Complementary Studies
- Cardiac profile: CPK 1407 | CK-MB 196.1 | Troponin I 1800.
- Lipid profile: Total cholesterol 127.5 | Triglycerides 107.6.
- Metabolic profile: Glucose 216.3 | TB 0.64 | DB 0.34 | IB 0.3 | AST 117.6 | ALT 70.3 | ALP 101 | Total Protein 6.2 | LDH 327 | GGT 88.
- Serum electrolytes: Na 133 | K 4.44 | Cl 101 | Ca 8.34 | P 3.76 | Mg 2.1.
- Blood chemistry: BUN 27.33 | Urea 58.6 | Serum Creatinine 1.0.
- Complete blood count: Leukocytes 20.6 | Neutrophils 13.7 | Lymphocytes 3.24 | Hb 17.3 | Hct 52.9 | Platelets 346,000.
Left Anterior Descending Artery (LAD)
Right Coronary Artery (RCA)
Rationale
Acute myocardial infarction (AMI) remains one of the leading causes of morbidity and mortality worldwide. Its most common pathophysiological mechanism is acute coronary occlusion secondary to thrombosis over a ruptured atherosclerotic plaque. However, simultaneous thrombosis in two or more coronary arteries is an uncommon entity associated with high mortality.
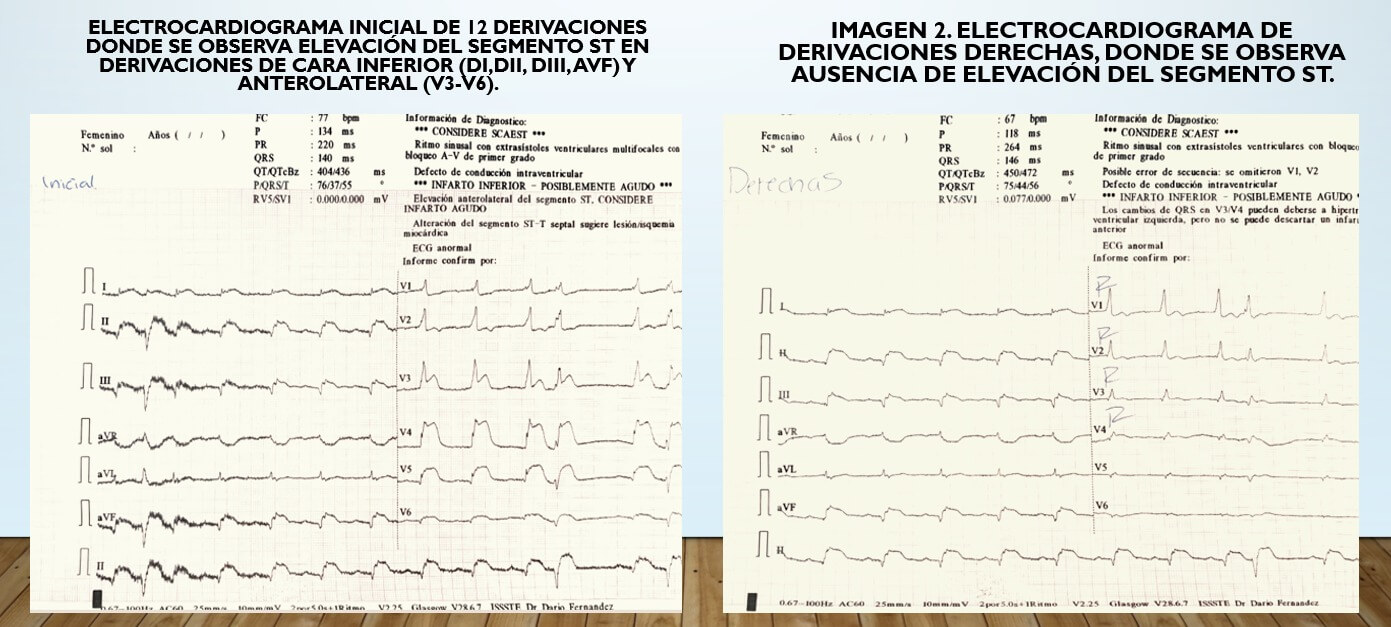
Recognizing this condition represents a true diagnostic challenge, as electrocardiographic findings may suggest involvement of multiple territories or an extensive lesion capable of masking another concomitant occlusion. Multivessel coronary occlusion is associated with hemodynamic instability, cardiogenic shock, and potentially fatal ventricular arrhythmias, requiring early diagnosis and an immediate revascularization strategy.
We present the case of a male patient with acute myocardial infarction secondary to simultaneous occlusion of the left anterior descending artery and the right coronary artery, progressing to cardiogenic shock refractory to treatment.
Join the Discussion – What Would You Have Done?
Before reviewing the case resolution—available below—we invite you to participate in the discussion by answering the following multiple-choice questions.
Case Resolution
Therapeutic Management
In this patient, the decision was made to treat both arteries during the same procedure due to hemodynamic deterioration and the development of cardiogenic shock. Unlike hemodynamically stable patients—in whom guidelines generally suggest a staged approach—immediate and complete revascularization was chosen in this scenario.
Initially, angioplasty with stent implantation was performed on the left anterior descending artery, followed by angioplasty of the right coronary artery. In addition, glycoprotein IIb/IIIa inhibitors, dual antiplatelet therapy, and unfractionated heparin were administered.
Rationale for the Decisions
- The culprit artery supplying the myocardial territory at greatest risk should be treated first.
- Multiple thromboses in STEMI patients are uncommon, and most available evidence comes from isolated case reports, making it difficult to establish uniform treatment strategies.
- Revascularization in the shortest possible time is essential, as these patients require immediate reperfusion therapy and intensive pharmacological treatment to improve prognosis.
Clinical Course and Outcomes
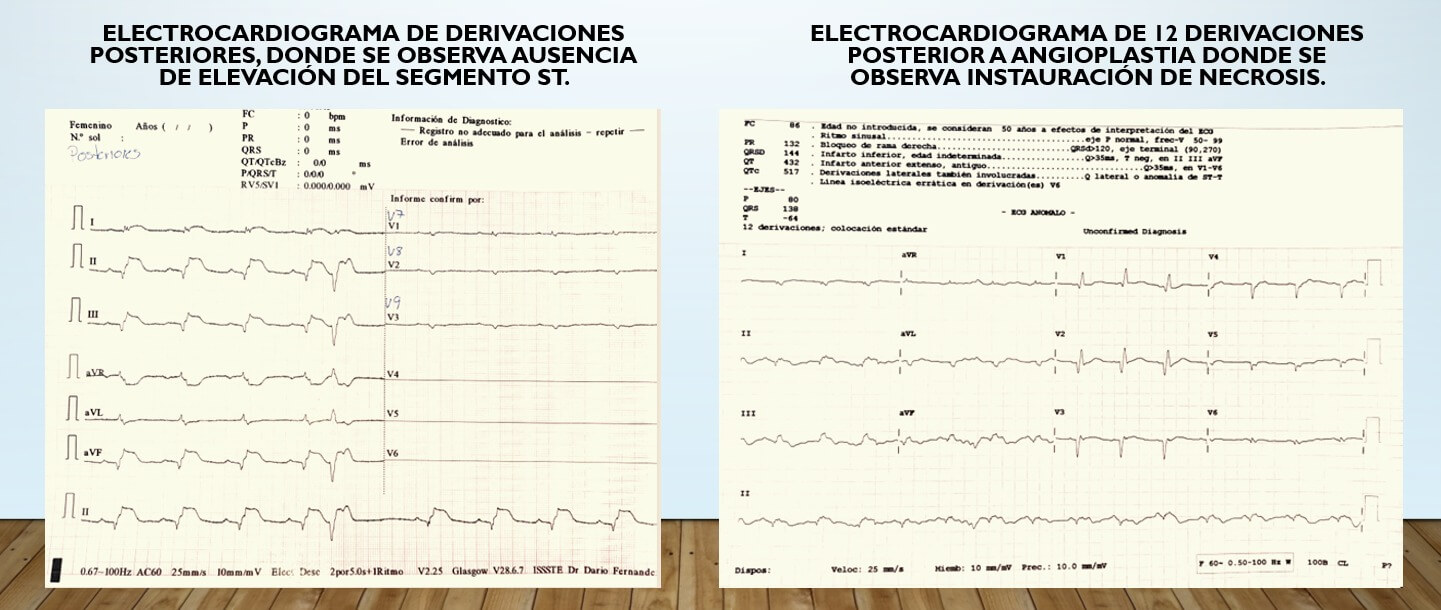
On the post-procedural control electrocardiogram, ST-segment resolution was observed, with evidence of necrosis in the leads initially affected.
Despite this, the patient remained hemodynamically unstable and developed refractory cardiogenic shock. Five hours after the procedure, he experienced cardiorespiratory arrest, without return of spontaneous circulation despite advanced resuscitation efforts.
Thank You for Reading!
We invite you to share your opinion about this case in the comments and join the discussion with the community.



{kind=link}