

Both fenestrated and branched endografts are effective to treat patients after failure of their initial endograft due to significant type I endoleak. This situation is costly both because of the devices themselves, and also due to the several endovascular and surgical procedures required.
Failure of an endograft to treat an infrarenal abdominal aortic aneurysm due to the development of a type Ia endoleak exposes patients to pressurization of the sac, which may cause a rupture. Type I endoleaks must undoubtedly be treated—unlike type II endoleaks, around which controversy may arise.
The purpose of this study was to evaluate the results of fenestrated/branched grafts for the treatment of type Ia endoleaks.
Between 2010 and 2019, 85 consecutive patients who received a fenestrated/branched graft after failure of a conventional prosthesis were included. The primary endpoint was freedom from re-intervention and death related to the procedure.
In 30 cases (35%), the initial prosthesis was implanted in a hostile neck—either too short (<10mm) or angled (>60°). Less frequent reasons were poor placement of the initial prosthesis, sizing error, or stent migration.
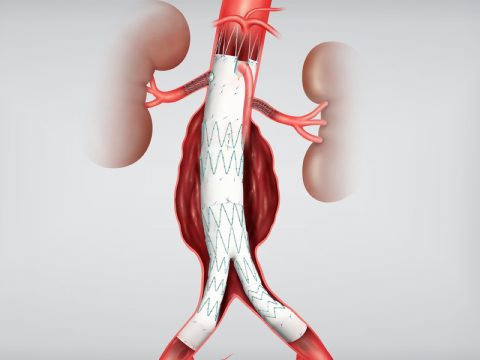
Type Ia endoleaks were observed 59 ± 25 months following implantation of the initial prosthesis. As a solution, 82 fenestrated grafts and 3 branched grafts were used. Overall technical success was 94%, with one persistent type Ia endoleak, and two unsuccessful stent graft implantations.
In-hospital mortality rate was 5%, and the most feared complication in this type of procedure—spinal cord ischemia—occurred in four patients.
At three years, the survival rate was 64% with an overall freedom from any re-intervention or aneurysm-related death of 40%. However, the secondary patency rate of the target visceral arteries was 96%.
Despite all efforts, six patients had to undergo conventional surgery.
Conclusion
Fenestrated/branched grafts are an effective treatment when conventional prostheses fail due to type 1A endoleak, although re-interventions and device costs can be high.
Original title: Prospective Multicentre Cohort Study of Fenestrated and Branched Endografts After Failed Endovascular Infrarenal Aortic Aneurysm Repair with Type Ia Endoleak.
Reference: Aurélien Hostalrich et al. Eur J Vasc Endovasc Surg. 2021 Aug 4;S1078-5884(21)00525-6. Online ahead of print. doi: 10.1016/j.ejvs.2021.06.019.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



{kind=link}