

Takayasu arteritis (TAK) is an uncommon granulomatous large-vessel vasculitis that affects the aorta and its primary branches.

The most frequently types of observed vascular compromise are obstructive lesions, and aneurysmal vascular lesions or dissections. In 2021, the American College of Rheumatology recommended not to implement percutaneous intervention (PI) with these patients and only use immunosuppressive therapy.
Joseph, G. et al., from Christian Medical College in Vellore (India), presented one of the largest series of patients with TAK in the world, with which they aimed at prospectively assessing TAK procedures and analyzing early and late outcomes.
Most patients were treated with a corticoid drug and a second-line agent (mycophenolate), while biologic agents (such as tocilizumab) were used in refractory cases.
PI was the treatment of choice for cases with symptoms, hemodynamically significant lesions, or severe lesions (≥70% stenosis, ≥5-cm diameter for fusiform aortic aneurysms, or high-risk complications). After treatment, interventions were classified as successful (<50 residual lesion), suboptimal (50%-69% residual lesion), and failure (≥70% residual lesion). Moreover, for aneurysms and dissections, interventions were defined as successful if the aneurysm was excluded or if there were no endoleak or complications.
Read also: Real-World Revascularization Strategy for Left Main Coronary Artery: Surgery or PCI?
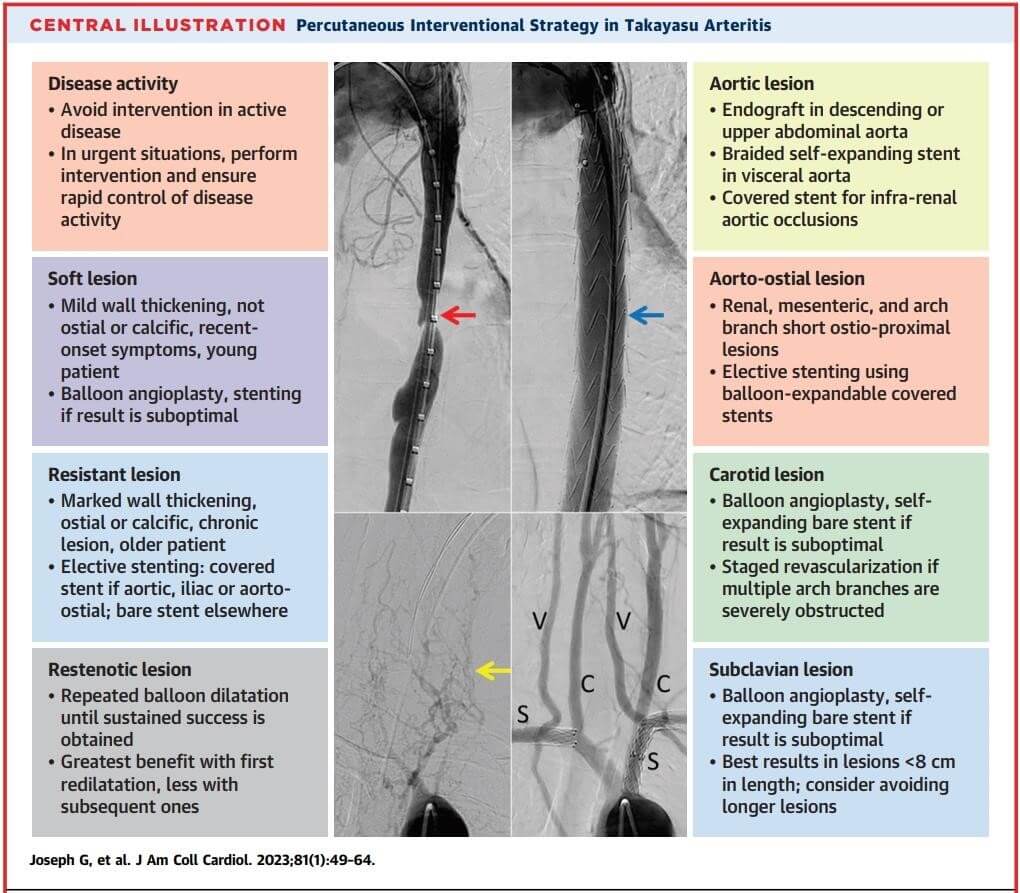
Obstructive lesions were treated with elective stenting (directly or with predilation), balloon angioplasty (BA), cutting-balloon angioplasty (CB), and—in cases with suboptimal outcome—eventual stent placement. Bare-metal stents (BMS), covered stents (CS), and drug-eluting stents (DES) were mainly used in the coronary area, whereas endografts were used in large aortic lesions.
Over 26 years (1996-2022), 1149 patients with a TAK-compatible angiography were included in the cohort. Then, patients with advanced vascular compromise (n = 942) were treated with PI; a total of 2450 lesions were treated (2.6 lesions per patient), of which 2365 were obstructive lesions and 85 were aneurysms or dissections. Location was mainly subclavian artery (630), renal artery (586), aorta (463), and carotid artery (333), among others. These lesions were treated with a total of 3805 PI procedures (1.55 PI per lesion); early success was obtained for 92.3% of the lesions and late success was achieved for 84.5% of them, with 39 months of follow-up.
There was increased success with repeat PI in obstructive lesions with restenosis (48% in the first intervention and 83% in the last one). Patients who underwent direct stenting had better early success when compared with those who underwent previous predilation.
Covered stents were more effective in the long-term follow-up (92.4 %) when compared with bare-metal stents (86.4 %; P = 0.009). Covered stent restenosis tended to occur focally at the distal stent edge, while bare-metal stent restenosis tended to be diffuse.
After analyzing specific affected segments, aortic and iliac lesions had a better late success index (≥90%). Moreover, repeat intervention in these areas was mainly scaffolded instead of due to restenosis (mainly using covered stents to apply high pressure when dilating).
Subclavian lesions were mainly treated with balloon angioplasty, obtaining better results in <8-cm lesions. Coronary lesions had a good early success index, which decreased in the long term (72%), mainly using drug-eluting stent.
Read also: Invasive Myocardial Viability Indexes.
Persistently increased disease activity (measured by biomarkers) was a strong restenosis predictor during follow-up.
Out of the 44 deaths observed during follow-up, one third were related to the procedure, and intracranial bleeding (due to hyperperfusion following recanalization) was the main complication (60%).
Conclusions
Researchers presented the largest cohort of TAK patients who underwent PI. In this population, it was proven that percutaneous treatment in most significant vascular lesions can be feasible, effective, safe, and durable. This demonstrates that PI can be a useful option for obstructive lesions (with 50% chances of it being a scaffolded procedure that should be repeated). Moreover, this study aims at widening interventionist options for patients with advanced vasculopathy due to TAK.

Dr. Omar Tupayachi.
Member of the Editorial Board of SOLACI.org.
Original Title: Outcomes of Percutaneous Intervention in Patients With Takayasu Arteritis.
Reference: Joseph, George et al. “Outcomes of Percutaneous Intervention in Patients With Takayasu Arteritis.” Journal of the American College of Cardiology vol. 81,1 (2023): 49-64. doi:10.1016/j.jacc.2022.10.024.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



{kind=link}