

The 2026 ACC/AHA guideline for the management of acute pulmonary embolism (PE) introduces a conceptual shift by replacing the traditional “risk-based” classification with an integrative system of clinical categories known as the Acute Pulmonary Embolism Clinical Categories (A–E).
This model incorporates clinical severity, biomarkers, right ventricular (RV) imaging, hemodynamic parameters, and respiratory compromise, shifting the focus from anatomical clot burden to physiopathological impact.
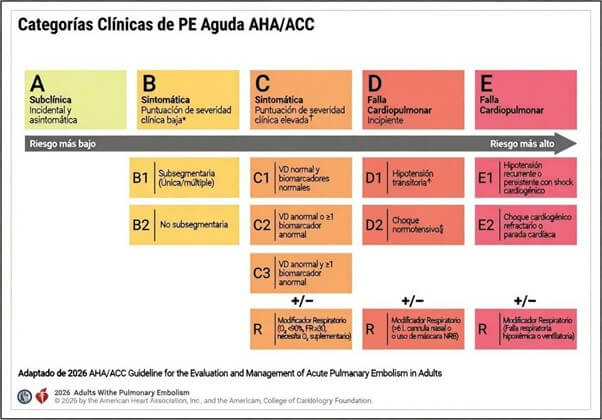
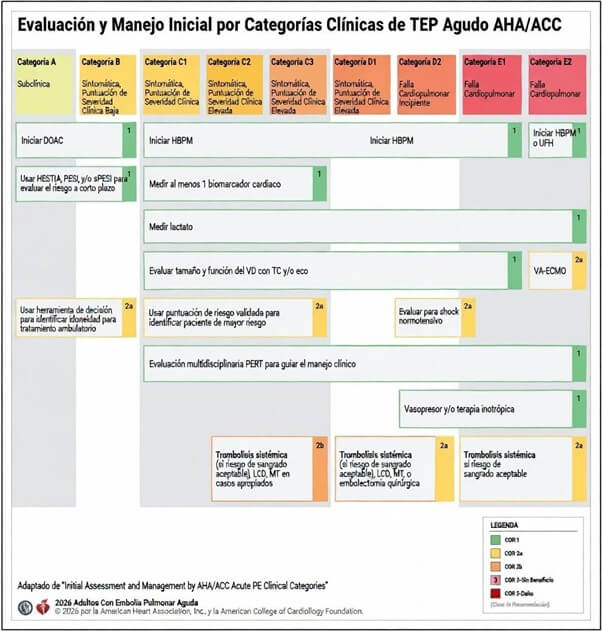
Categories A and B identify patients with low clinical severity. In these scenarios, the guideline considers outpatient management reasonable, provided there is immediate access to anticoagulation and structured follow-up. Direct oral anticoagulants (DOACs), in the absence of contraindications, facilitate this strategy.
Category C includes patients with high clinical severity (PESI III–V, sPESI ≥1, or Hestia ≥1), with or without cardiopulmonary dysfunction. In prior ESC guidelines, this group corresponded to the traditional “intermediate-risk” category, now further subdivided according to the degree of functional impairment.
A distinctive contribution is Category D, which defines “incipient cardiopulmonary failure” and formally incorporates the concept of normotensive shock. It is subdivided into:
D1: transient or relative hypotension responsive to fluids, without hypoperfusion or organ damage.
D2: normotensive shock.
Thrombus Burden: Anatomy Does Not Define Early Risk
The guideline establishes that quantification of thrombus burden should not be used for risk stratification in Categories A–C (Class 3: No Benefit). Evidence demonstrates no association between thrombus burden and adverse events after excluding patients with a shock index greater than 1. The message is clear: therapeutic decisions should be based on hemodynamic impact rather than isolated anatomical extent.
Right Ventricle–Oriented Hemodynamic Support
In Categories D–E, hemodynamic stabilization is a priority. Norepinephrine is the vasopressor of choice to maintain mean arterial pressure and RV coronary perfusion. In selected cases, vasopressin may be added as a second-line agent.
In the presence of low cardiac output and significant RV dysfunction (E1–E2), dobutamine may be used to improve contractility, with close monitoring due to its potential systemic vasodilatory effects. In normotensive shock, it may be considered as an initial strategy.
The guideline acknowledges the use of inhaled vasodilators, such as nitric oxide or prostacyclins, to reduce pulmonary vascular resistance and optimize RV–pulmonary artery coupling.
Regarding respiratory support, invasive mechanical ventilation should be avoided whenever possible, favoring high-flow nasal cannula or noninvasive ventilation. The guideline also warns about the risks of deep sedation, even in normotensive patients, due to the potential for circulatory collapse secondary to inhibition of physiological compensatory mechanisms.
Lea también: ¿Puede realizarse el TAVI de forma segura en pacientes con válvula aórtica bicúspide?
In refractory shock, venoarterial extracorporeal membrane oxygenation (VA-ECMO) is reasonable when adequate resources and expertise are available, with the aim of stabilizing hemodynamics and improving oxygenation.
Catheter-Based Therapies and Mechanical Thrombectomy
The guideline clearly delineates the interventional space. In Category E1, catheter-directed thrombolysis (CDT) plus anticoagulation is reasonable (Class 2a) to prevent clinical deterioration and early mortality.
In D1–D2, CDT may be considered in selected patients with progressive deterioration.
Regarding mechanical thrombectomy (MT), in E1 it is reasonable (Class 2a) compared with anticoagulation alone to prevent further decompensation and early mortality; in D1–D2, it may be considered.
In Category C, the benefit remains uncertain, and its use should be restricted to patients with clinical progression, following multidisciplinary decision-making within a structured Pulmonary Embolism Response Team (PERT).
Conclusions
Reference: Writing Committee Members*; Creager MA, Barnes GD, Giri J, Mukherjee D, Jones WS, Burnett AE, Carman T, Casanegra AI, Castellucci LA, Clark SM, Cushman M, de Wit K, Eaves JM, Fang MC, Goldberg JB, Henkin S, Johnston-Cox H, Kadavath S, Kadian-Dodov D, Keeling WB, Klein AJP, Li J, McDaniel MC, Moores LK, Piazza G, Prenger KS, Pugliese SC, Ranade M, Rosovsky RP, Russo F, Secemsky EA, Sista AK, Tefera L, Weinberg I, Westafer LM, Young MN. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026 Feb 19. doi: 10.1161/CIR.0000000000001415. Epub ahead of print. PMID: 41712677.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



 agudo introduce un cambio conceptual al reemplazar la clasificación tradicional “según riesgo” por un sistema integrador de categorías clínicas denominado Acute Pulmonary Embolism Clinical Categories (A–E).){kind=link}