

A recent presentation at London Valves took a closer look at the REPRISE III trial as regards two points that generated much discussion, such as need for a pacemaker and paravalvular leak.
REPRISE III had previously demonstrated that the Lotus is noninferior to first-generation CoreValve and Evolut R in terms of safety. Additionally, it proved to be superior for the primary efficacy combined endpoint at 1 year (death, disabling stroke, and moderate or greater paravalvular leak).
Read also: “Impella Improves Safety in High Risk Unprotected Left Main PCI”.
The definition of the REPRISE III composite safety endpoint did not include need for a pacemaker, which was stuck at 35.5% with Lotus vs. 19.6% for the combined both-generation CoreValve group (p < 0.001).
On the other hand, the composite efficacy endpoint was basically driven by the reduction in moderate/severe leaks (2% vs. 11.1%; p < 0.001).
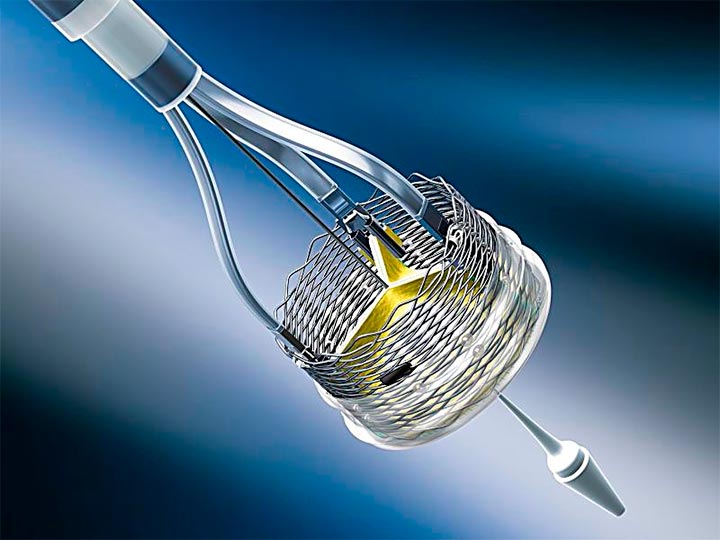
The Lotus valve is specifically designed for highly calcified disease anatomies, thanks to its repositionability and its small cell frame that conforms to rigid calcium structure. On the other hand, its adaptive urethane seal conforms to irregular surfaces.
Read also: “Small Annulus: Should We Start Choosing the Valve?”
Patients were categorized by calcium load observed in the computerized tomography scan across three tertiles (calcium in the leaflets, annulus, and outflow tract); ≥795.3 mm3 were considered as severe calcification. A total of 98 out of 297 CoreValve patients presented severe calcification, and so did 195 out of 577 patients in the Lotus valve group.
At 1 year, moderate/severe paravalvular leak was significantly greater among patients who received the CoreValve device and presented severe calcification vs. Lotus patients. This difference was not observed in the two tertiles with lower calcium burden.
These data might suggest that transcatheter aortic valve replacement (TAVR) with the Lotus valve may be more beneficial in treating patients with severe calcification than other valves.
Most patients who required a pacemaker after Lotus implantation needed it due to third-degree atrioventricular block or Mobitz Type 2, and this did not affect clinical results or patient quality of life.
Implantation depth was a key predictor of need for a pacemaker, and perfecting the Lotus implantation technique reduced the overall number of pacemakers required. However, this difference was not statistically significant.
A 30% rate of need for a pacemaker with Lotus does not seem to be acceptable now that TAVR is moving towards intermediate- and low-risk populations.
The end of this story will be told by the new Lotus Edge, which incorporates a depth guard system that might lower the pacemaker implantation rate from 30% to 10%.
Original title: The Impact of Calcium Burden on Clinical Outcomes and Paravalvular Regurgitation in the REPRISE III Randomized Controlled Clinical Trial.
Reference: Makkar R et al. Presented at: PCR London Valves 2017. September 25, 2017. London, England.
Get the latest scientific articles on interventional cardiologySubscribe to our weekly newsletter
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}