

The mitral valve is a complex apparatus dependent on left atrium and left ventricle functionality. Dilation of these cavities might affect mitral annulus morphology and lead to valve dysfunction, generating mitral regurgitation (MR). This type of MR has been called functional, since leaflets and tendinous chordae do not present lesions themselves; instead, they malfunction ‘secondary’ to either atrium or ventricle annulus dilation.
 After the promising outcomes of the EVEREST I and II trials and their registry (mostly based on patients with degenerative MR), the use of the MitraClip device has become more and more massive, currently reaching > 60,000 implantations. Different registries have been including a growing number of functional MR cases (FMR). Outcomes would indicate that patients benefit from these devices, since they showed improved functional capacity, reduced number of hospitalizations and improved 6-minute walk tests. However, the first and only randomized study to compare maximally tolerated guideline-directed medical therapy (GDMT) against GDMT + MitraClip in patients with FMR, recently published, had shown negative outcomes for the MitraClip, with apparently no benefits for patients.
After the promising outcomes of the EVEREST I and II trials and their registry (mostly based on patients with degenerative MR), the use of the MitraClip device has become more and more massive, currently reaching > 60,000 implantations. Different registries have been including a growing number of functional MR cases (FMR). Outcomes would indicate that patients benefit from these devices, since they showed improved functional capacity, reduced number of hospitalizations and improved 6-minute walk tests. However, the first and only randomized study to compare maximally tolerated guideline-directed medical therapy (GDMT) against GDMT + MitraClip in patients with FMR, recently published, had shown negative outcomes for the MitraClip, with apparently no benefits for patients.
Read also: What to Do with Blood Pressure Levels Between 130/80 and 139/89 mmHg.
We could review this extensively, but we will only look at a few limitations, and compare its outcomes against the COAPT trial. We will mention the low number of patients (152 patients per branch) which has low statistical power, crossover of patients between branches, unsatisfying immediate outcomes (>25% patients with MR 3-4), the big number of patients with moderate MR, and important left ventricle deterioration (ejection fraction 15-40%), among others.
Today, we are pleased to announce the COAPT outcomes, simultaneously published in the New England Journal of medicine and TCT/San Diego, which turned out to challenge the above mentioned study. This trial, conducted between December 2012 and June 2017 in 78 medical centers across Canada and the US, included 614 patients (302 in the MitraClip group and 312 in the GDMT group) with cardiac failure and FMR > to moderate, in two branch treatments, GDMT and GDMT + MitraClip. Eligible patients presented cardiomyopathy (ischemic 60.7% or non-ischemic 39.3%) with 20-50% LVEF, secondary MR (degree 3+ or 4+), symptomatic [NYHA] functional class II, III or IV, ambulatory despite stable maximally tolerated GDMT regime per guidelines, and cardiac resynchronization therapy, if indicated. STS score predicted high surgical risk (mean 7.8±5.5 for the MitraClip group, 8.5±6.2 for the GDMT group).
Read also: Aortic Stenosis with Normal Flow Low Gradient: Should We Intervene or Wait?
In the MitraClip group, successful implantation rate was 97%, with mean 1.7±0.7 implanted clips. At discharge, MR was 1+ or lower in 214 patients (82.3%), 2+ in 33 patients (12.7%), 3+ in 9 patients (3.5%) and 4+ in 4 patients (1.5%). Mortality and stroke rates at 30 days were 2,3% and 0,7% respectively, and no patients were submitted to mitral valve surgery. 97.7% of patients had available data at 1-year follow-up; mean follow-up was 22.7 months (interquartile range 12.4 to 24.0).
Results
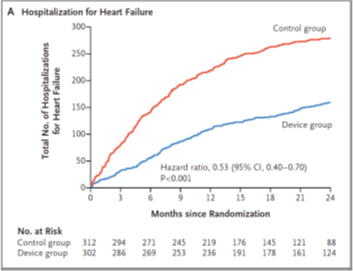
One or more hospitalizations due to cardiac failure occurred at follow-up in 92 patients in the MitraClip group, and in 151 in the control group.
Annual hospitalization rate (Table A) caused by cardiac failure was 35.8% per year in the MitraClip group, vs. 67.9% per patient-year in the control group (HR 0.53; CI 95%, 0.40 to 0.70; P <0.001).
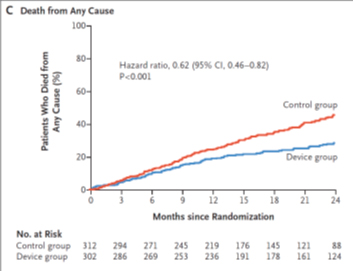
All-cause mortality (table C) at 2 years was significantly lower in the MitraClip group vs. GDMT alone (29,1% vs. 46,1%; HR 0,62; CI 95%, 0,46 to 0,82; p <0,001).
Functional capacity and quality of life were also significantly better with MitraClip.
Possible explanations for the differences with MITRA FR outcomes:
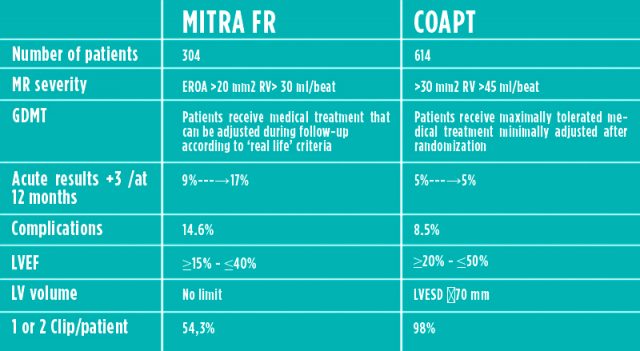
After looking at the table, the most important conclusion is that the COAPT trial selects patients far less evolved, uses more experienced operators, and practically the same medical treatment during follow-up.
Conclusion
Among patients with cardiac failure and secondary mitral regurgitation, moderate to severe or severe, that remain symptomatic despite the use of maximally tolerated medical treatment per guidelines, percutaneous repair with MitraClip resulted in lower hospitalization rate for cardiac failure and reduced mortality at 2-year follow-up.
Get the latest scientific articles on interventional cardiologySubscribe to our weekly newsletter
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.



{kind=link}