

In the era of endovascular intervention, with shorter revascularization times, we see lower rates of mechanical complications due to acute myocardial infarction (AMI). Increased rates were recorded during the COVID-19 pandemic, but driven by delays in consultation.

Though occasional (with an estimated incidence of 0.2%), post AMI ventricular septal defect (VSD), or interventricular communication, involves high mortality. Ischemic VSD will produce ischemia related disorders in addition to mechanically compromising the left-right shunt. Surgical repair with patch has been the preferred strategy for many years, though percutaneous closure is a valid strategy increasingly being used.
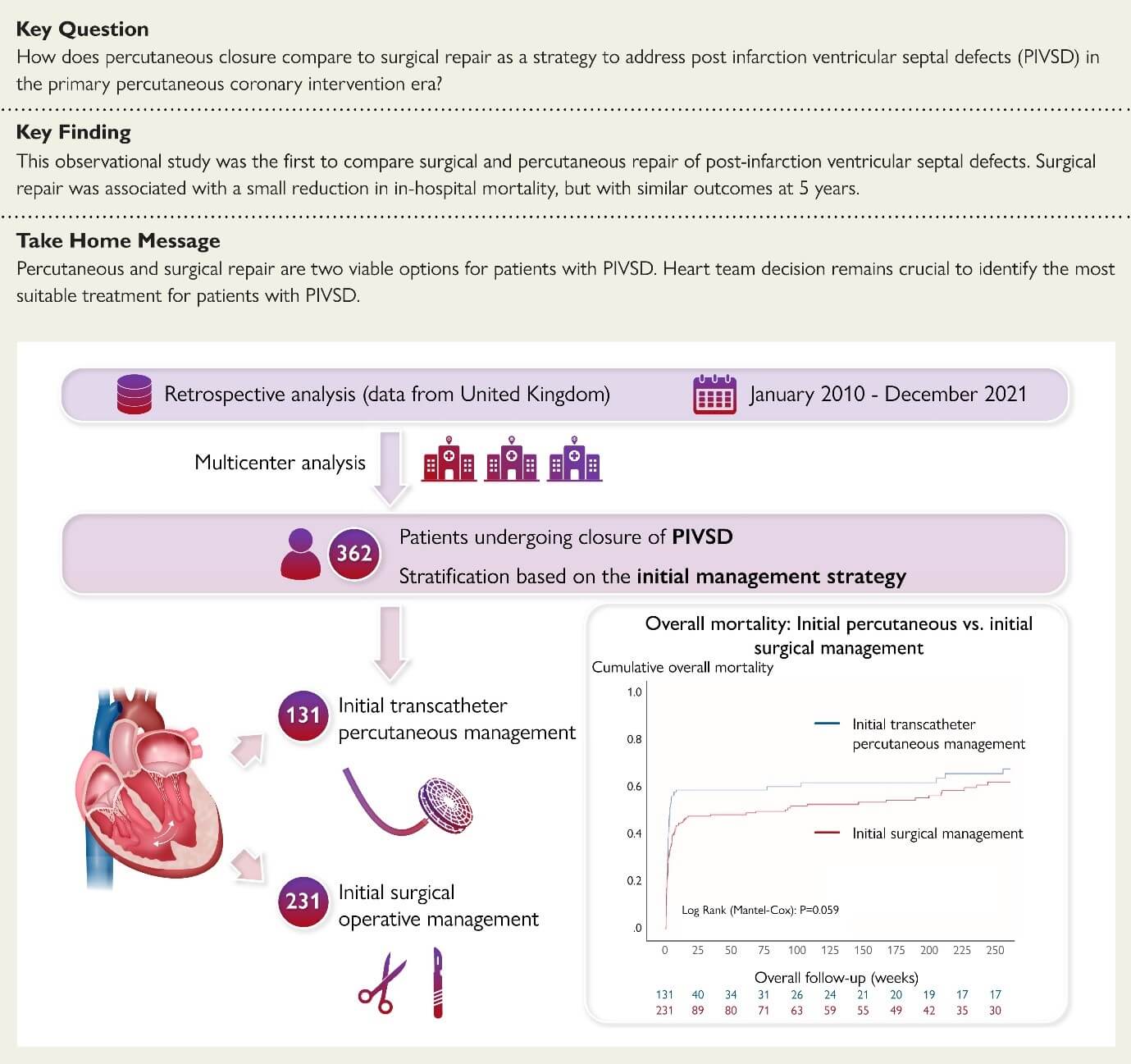
This observational retrospective study of a registry in the UK gathered data from patients with post AMI VSD since 2010, aiming at comparing inhospital vs long term mortality.
Data from 362 patients treated for post AMI VSD were in looked at, 231 were treated with surgery (93.4% patch) and 131 percutaneously (64% use of Amplatzer). Overall, patients treated with closure devices were older (72 vs 67 years; P<0.001) and had higher BMI (28 vs 26 kg/m2; P=0.01). On the other hand, surgical patients presented larger septum defects (18 vs 20mm, P<0.001) and were more often diagnosed with cardiogenic shock (51.9% vs 62.8%, P=0.044).
Read also: Stent Thrombosis: Clinical Characteristics and Event Predictors in a Contemporary Cohort.
13% of patients treated percutaneously required an additional procedure (either surgical or percutaneous). Also, there was high crossover: 15% of endovascular patients required surgery and 7.4% of surgical patients required a closure device.
In hospital mortality was 48.1%, with more events in the endovascular arm (55% vs 44.2%, P=0.048), whereas 5-year mortality saw no significant differences (61.1% vs 53.7%, P=0.17). Independent factors associated with mortality were cardiogenic shock (aHR 1.97, CI 95% 1.37-2.84; P<0.001) and initial percutaneous approach (aHR 1.44, CI 95% 1.01-2.05, P=0.042).
Conclusions
This study has shown that, despite the latest technological advance, mortality associated to ischemic VSD remains high, regardless the strategy. This study presents limitations because of high crossover. These patients should be treated either surgical or percutaneously, seeing as medical treatment alone rendered nearly 94% mortality rate.

Dr. Omar Tupayachi.
Member of the Editorial Board of SOLACI.org.
Original Title: Post-infarction ventricular septal defect: percutaneous or surgical management in the UK national registry.
Reference: Giblett, Joel P et al. “Post-infarction ventricular septal defect: percutaneous or surgical management in the UK national registry.” European heart journal, ehac511. 17 Sep. 2022, doi:10.1093/eurheartj/ehac511.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology



{kind=link}