

Share your experience. Learn from experts. Grow as an interventionalist.
We present the first case of this new edition of The Fellow’s Corner, an academic and collaborative space where fellows can share real clinical cases, exchange experiences, and discuss questions or challenges related to daily practice in cardiovascular intervention.
Below, we present a real-world clinical case, accompanied by a series of questions to explore how you would have acted. Finally, we will share the case resolution and the strategy adopted.
In this first installment, we address a scenario that undoubtedly represents a true challenge in clinical practice: “Chronic Total Occlusion Treated via Retrograde Approach.”
- Case Author: Dr. Alejandro González Véliz (Cuba)
- Institution: Institute of Cardiology and Cardiovascular Surgery, Havana, Cuba
- Head of Department: Dr. Leonardo H. López Ferrero
Table of Contents
Case Presentation: Chronic Total Occlusion Treated via Retrograde Approach
- Clinical data: 63-year-old male with cardiovascular risk factors including smoking and hypertension. Left ventricular ejection fraction (LVEF): 52%.
- Reason for admission: Progressive worsening angina.
- The patient has known coronary artery disease with a chronic total occlusion in the proximal segment of the left anterior descending artery (LAD), and a previous failed attempt at percutaneous coronary intervention (PCI) via the antegrade approach.
Coronary Angiography
- Right coronary dominance
- Left anterior descending artery: chronic total occlusion in the proximal segment, with an ambiguous proximal cap. J-CTO score: 2
- Presence of heterocoronary collateral circulation from inferior septal branches
Join the discussion: What would you have done?
Before reviewing the case resolution (available below), we invite you to take part in the discussion by answering the following multiple-choice questions.
Case Resolution
Final decision: Retrograde approach using wire escalation technique.
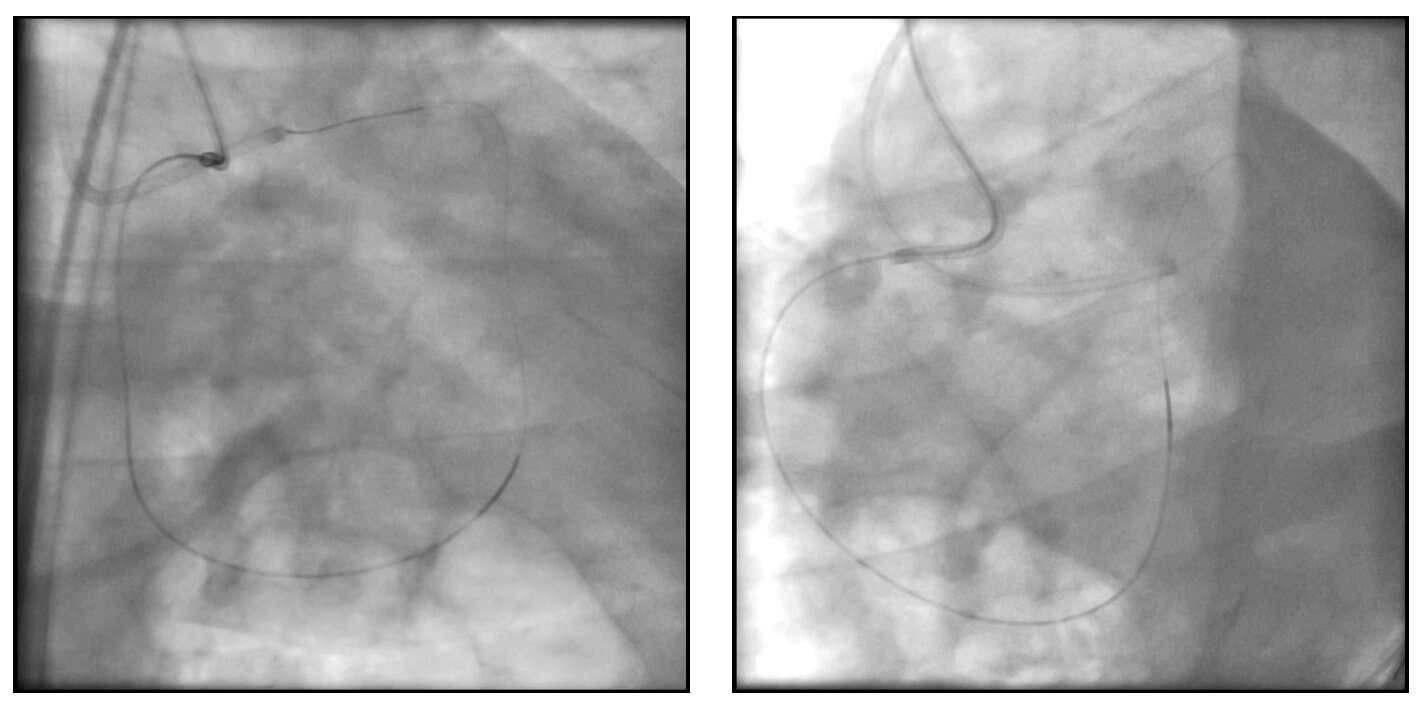
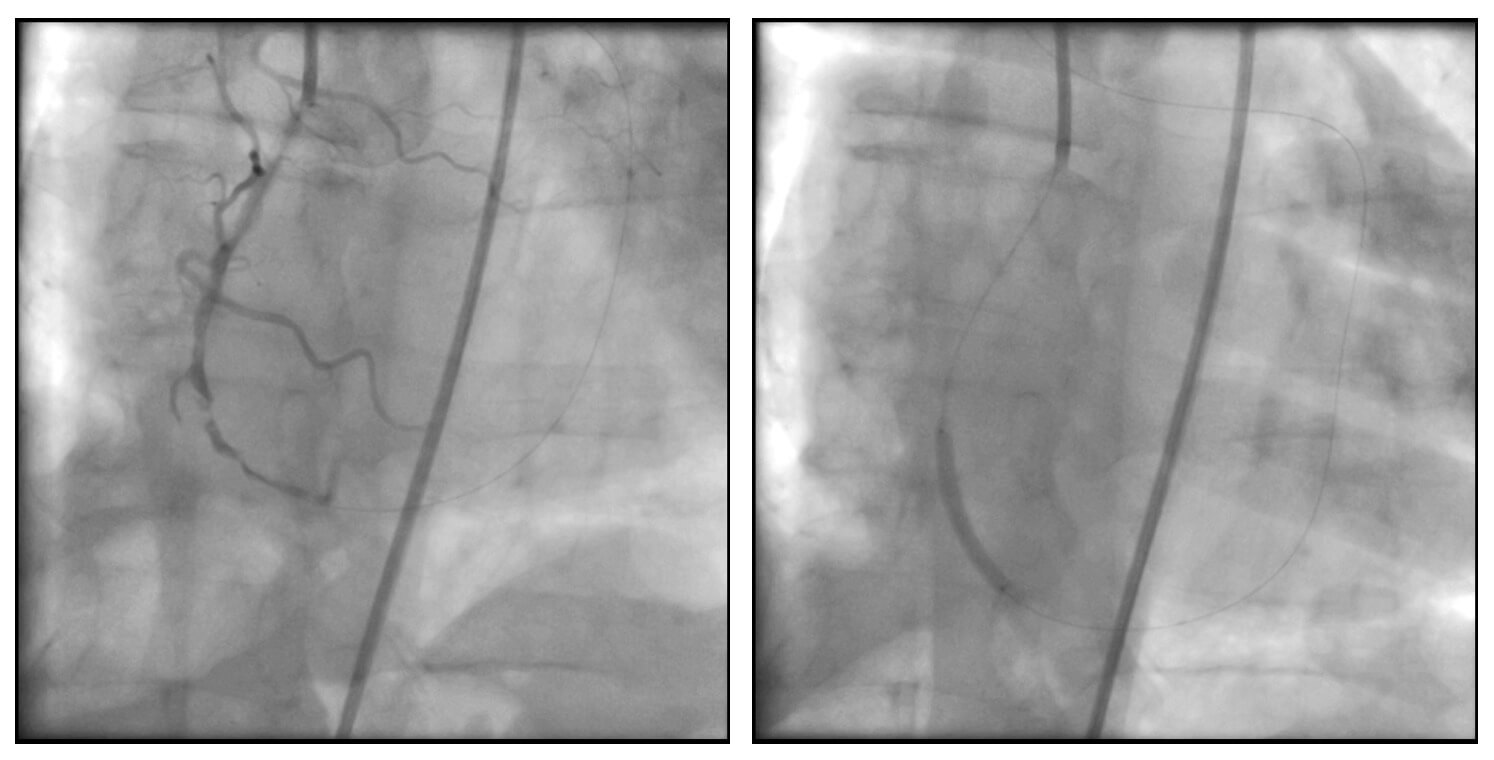
Dual contrast injection was performed in both coronary arteries (right coronary artery with an Amplatz Right catheter and left anterior descending artery with an EBU catheter). Werner classification: 2.
An Asahi Sion Black intracoronary guidewire was advanced from the right coronary artery through a septal collateral branch, reaching the mid segment of the left anterior descending artery, with support from a Turnpike microcatheter. The wire was then exchanged for a 300 cm wire for externalization through the catheter positioned in the left main coronary artery.
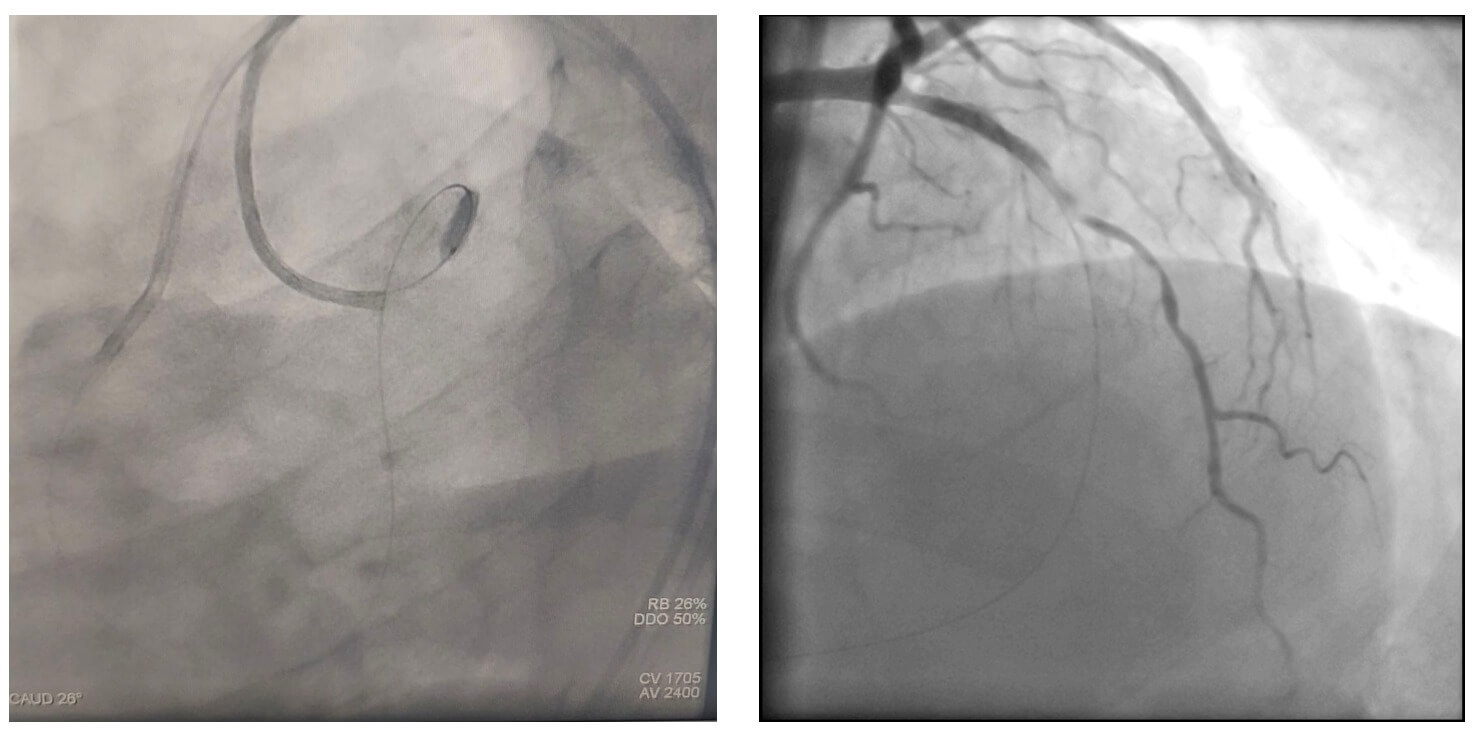
During wire externalization, the patient developed hemodynamic instability, and a coronary dissection of the right coronary artery was identified. A stent was implanted, resulting in clinical improvement and allowing continuation of the planned procedure.
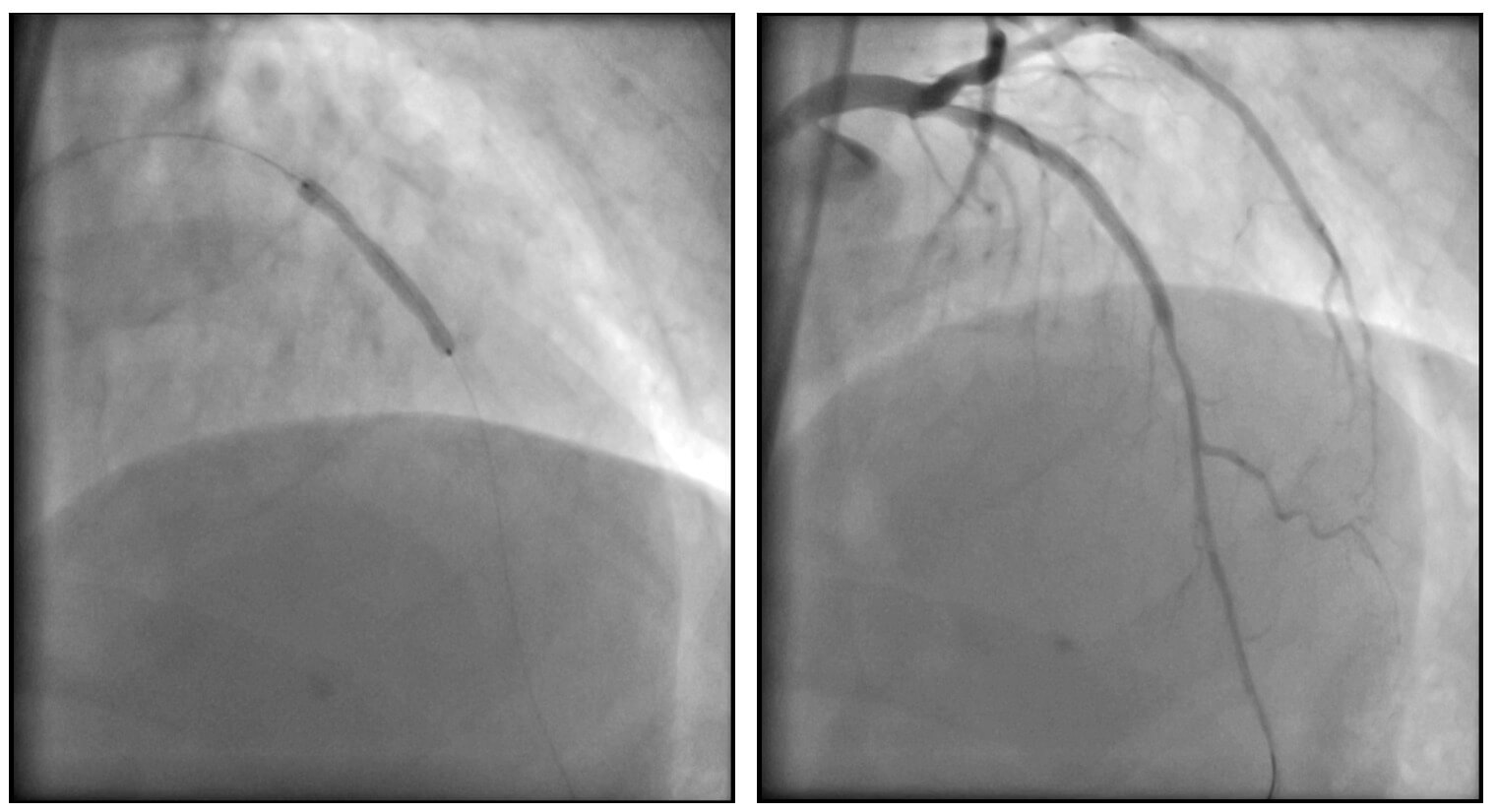
Subsequently, the occlusion was predilated using low-profile balloons, and a DEStiny stent was implanted at the lesion site. After vessel recanalization, a lesion was identified at the re-entry zone (site where the retrograde wire entered from the right coronary artery). An antegrade wire was advanced, and a second stent was implanted.
An excellent final angiographic result was achieved. The patient was discharged 48 hours after the procedure without complications.
Thank you for reading!
We invite you to share your opinion about this case in the comments and join the discussion with the community.



{kind=link}