Several cases have shown an association between patent foramen ovale and cryptogenic shock, particularly in patients under 55 and in those with atrial septal aneurysm or a significant right-to-left shunt.

Using PFO closure for stroke prevention has been controversial and, so far, no randomized studies have shown the superiority of this strategy compared to anti-thrombotic therapy.
To answer this question, the CLOSE study (Patent Foramen Ovale Closure or Anticoagulants versus Antiplatelet Therapy to Prevent Stroke Recurrence) randomized 664 patients in a 1:1:1 ratio to three arms and a mean 5.3±2.0 year follow up.
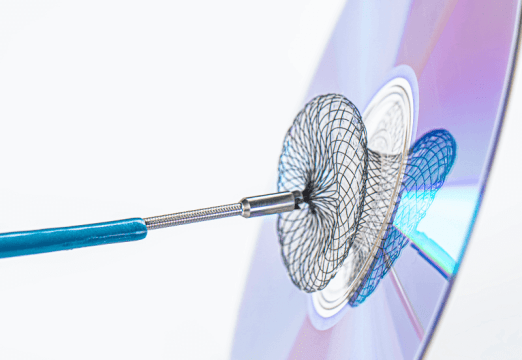
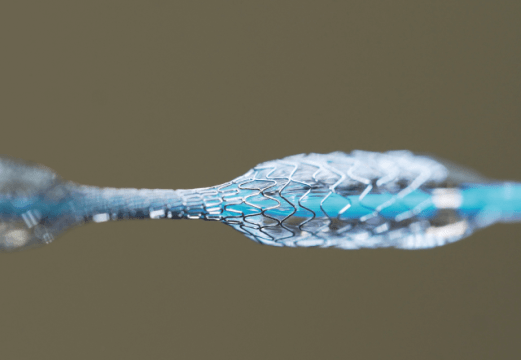
- One of the arms received transcatheter PFO closure followed by prolonged antiplatelet treatment (PFO closure group) or oral anticoagulation (anticoagulation group). This was randomization group 1.
- Patients with anticoagulant contraindication were randomized to PFO closure followed by prolonged antiplatelet treatment (PFO closure group) or to antiplatelet only treatment (antiplatelet treatment group). This was randomization group 2.
- Patients with PFO contraindication were randomized to anticoagulation (anticoagulation group) or to antiplatelet only treatment (antiplatelet only group). This was randomization group 3.
Read also: “REDUCE Trial: Patients with PFO and cryptogenic stroke at lower risk of recurrent stoke when treated with APT and closure device”.
Primary end point was stroke. The comparison of PFO closure plus antiplatelet therapy vs. antiplatelet only therapy was performed with combined data from randomization groups 1 and 2, and the comparison between oral anticoagulation vs. antiplatelet only therapy was performed with combined data from randomization groups 1 and 3.
In the analysis of randomization groups 1 and 2, no strokes were observed among the 238 patients in the PFO closure group, whereas 14 strokes were observed among the 235 patients in the antiplatelet only group (HR, 0.03; CI 95% 0 a 0.26; p<0.001). 5.9% of patients receiving PFO closure presented some kind of procedural complication and also showed a much higher rate of atrial fibrillation compared to the antiplatelet-only group (4.6% vs. 0.9%, P=0.02), even though the serious adverse events rate was similar in both groups.
Read also: “Results of the RESPECT Trial Bring About Excellent News”.
In the analysis of randomization groups 1 and 3, stroke was seen in 3 of 187 patients assigned to anticoagulants and in 7 of 174 patients assigned to antiplatelet only therapy.
Conclusion
In patients with recent cryptogenic stroke attributed to PFO associated with atrial septal aneurysm or significant right-to-left shunt, the rate of stroke recurrence was lower among those assigned to PFO closure combined with antiplatelet therapy vs. those assigned to antiplatelet only therapy. PFO closure was associated to higher incidence of atrial fibrillation.
Editorial Comment
This study did not have enough statistical power to compare the anticoagulation group to the antiplatelet only group, which is why it does not look into the statistical significance between these groups.
The risk of stroke at 5 years according to Kaplan–Meier is almost 5 points lower with PFO closure, which means avoiding 1 stroke at 5 years every 20 patients treated.
Most strokes in the antiaggregation group occurred in patients presenting PFO and septal aneurysm, which matches all prior observational studies.
Original title: Patent Foramen Ovale Closure or Anticoagulation vs. Antiplatelets after Stroke.
Reference: Mas JL et al. N Engl J Med. 2017 Sep 14;377(11):1011-1021.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology
We are interested in your opinion. Please, leave your comments, thoughts, questions, etc., below. They will be most welcome.