In the transcatheter aortic valve replacement (TAVR) session we had a presentation by Dr. John P. Vavalle (USA), head of the Structural Heart Disease Program at the University of North Carolina at Chapel Hill.
In his presentation, he showed how far the limits of percutaneous aortic valve implantation can be stretched by briefly showing successful cases:
- A first case with a very large annulus >900 mm2 treated with a 29-mm Sapien S3 valve.
- A second case of pure aortic regurgitation without calcification in the annulus with implantation of a 26-mm S3 valve.
- A third case of extreme tortuosity with bilateral Lunderquist guidewire placement. He was able to perform the procedure with a long hydrophilic introducer and a snare advancement system.
- Dr. Vavalle closed the session with a case of very horizontal aorta in which he emphasized the importance of performing aggressive valvuloplasties and having deflectable delivery systems.

He later made a presentation on TAVR in bicuspid valves.
In this regard, he commented on the growth of the transcatheter strategy in bicuspid valve patients according to the TVT Registry.
Also, an analysis conducted by Dr. Makka et al showed that, compared with tricuspid valve patients, there were no differences in death, stroke, paravalvular leak or complications of the procedure, which evidences the efficacy of TAVR. Dr. Vavalle emphasized that these analyses included very select patients (with a very favorable anatomy for TAVR) that differ from those found in clinical practice. Consequently, he mentioned the importance of waiting for long-term results on this.
The correct characterization of bicuspid valve anatomy is important, noting that those patients with calcified raphe and leaflets had much worse prognosis. We should always take into account the size and shape of the annulus, which is usually accompanied by low, anomalous coronary birth.
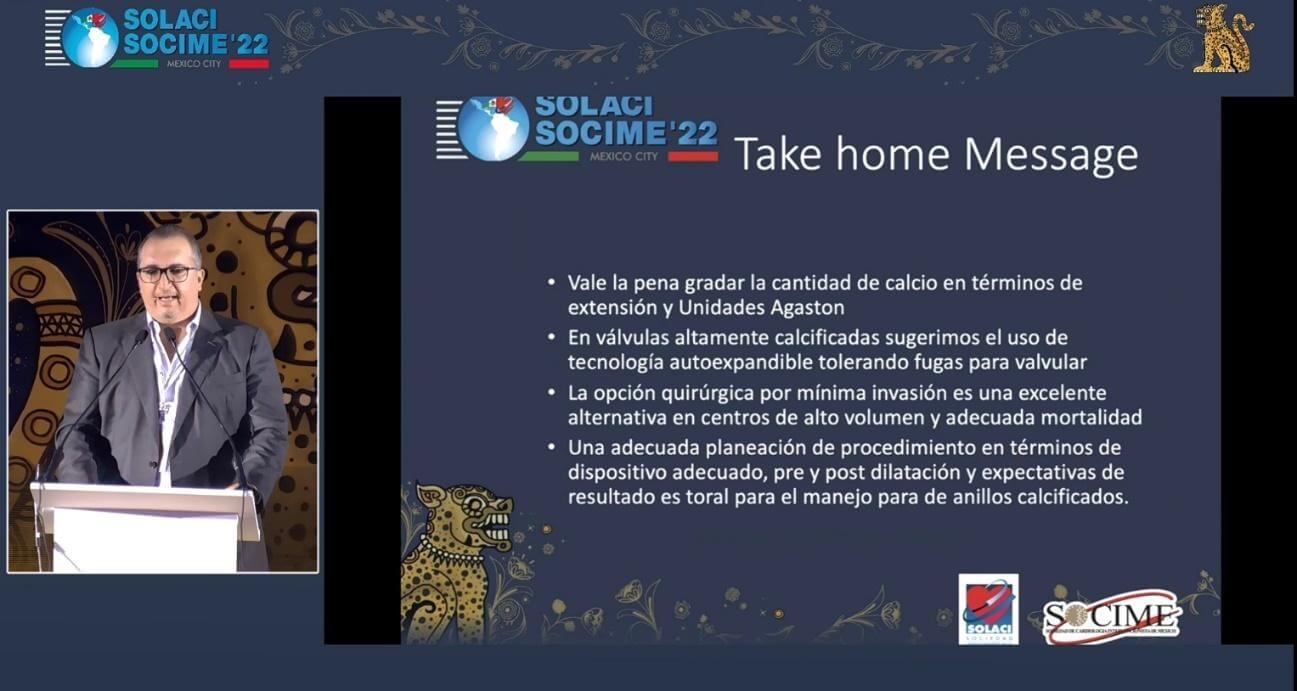
Afterwards, Dr. Jose Merino (MEX) spoke about TAVR in calcified annulus and analyzed the increased treatment complexity, observing complications such as paravalvular leak, conduction abnormalities, annulus rupture, and risk of coronary occlusion.
How should we plan with a patient with severe valvular calcification? Evaluate the calcium load, its asymmetry, and extension both to the aortic root and the left ventricular outflow tract, as well as in the landing zone.

Dr. Omar Tupayachi.
Member of the Editorial Board of SOLACI.org.
Subscribe to our weekly newsletter
Get the latest scientific articles on interventional cardiology